
Two weeks ago we had unusual patient in our office. The patient in her early fifties and very fit. Four years ago she did a lot of step aerobics and started to have pain on the bottom of the right foot. She continued to exercise until she started to feel pain in the left foot. From that point her pain continued to increase despite of all therapies she tried.
She worked with 4 different podiatrists, she had three steroid injections, she tried acupuncture, stretching. Three (!) custom orthotics were made for her with total cost of $1500 and they only made her foot pain worse.
Her recent foot X-ray ruled out calcaneal spur on either foot. Currently she stays away from exercise and she feels pain all day long. The pain is mostly located in the ball of feet while she was standing or she felt it throbbing at rest if she spent a lot of time on her feet.
The initial evaluation showed that she indeed has classic picture of the Plantar Fasciitis. The puzzling was the fact that for so long and despite of all correct treatment options the clinical picture didn’t improve but got worse.
Examination of the foot itself at least partly explained this. Picture below shows two right feet.

Left picture shows the plantar fascia (red arrow) of the average foot when greater toe passively extended. Right picture shows our patient’s foot. The difference is striking, the plantar fascia (red arrow) in our patient is under such tension that it is almost entirely exposed as a cord directly under the skin. The pressure in this string was so high that one can snap it back and forth like on a string.
It is impossible to say at this point if it was her inborn foot structure or tension developed as a pathology later after years of pain and unsuccessful therapies.
Surprisingly she had just moderate pain and tension when direct pressure was applied along plantar fascia. The mild symptoms didn’t fit into picture of acute Plantar Fasciitis which suppose to be cause of her pain. Such moderate clinical picture in the combination with unsuccessful therapies made us curious about real trigger of her pains. Detailed examination of her feet indicated two important findings presented in pictures below:
1. As we mentioned above the examination of plantar fascia revealed moderate tension all way to the heads of metatarsal bones with formed ball of the foot (left picture) when strictly vertical pressure (red arrow) applied to the fascia at its insertion to the head of metatarsal bone.

However when angle of pressure was changed (red arrow) to the direction of the metatarsal heads (right picture) the patient practically jumped from the table and she shouted that this is exactly pain she felt no one until now was able to find its exact location.
This finding means that plantar fascia lost its elasticity and by itself doesn’t trigger pain sensations because it partly scarificated. The pain she felt in the ball of foot came from the periostal trigger points developed in the heads of metatarsal bones and that was real cause of her pains.
2. Direct application of pressure along the plantar fascia didn’t trigger severe foot pain. As it was shown in first picture greater toe extension exposed plantar fascia. Black arrows emphasized points of pressure. Just from professional curiosity we decided to examine part of the plantar fascia which is normally inaccessible. Using tip of the index finger (picture below) we got on the inner surface of the plantar fascia and applied very moderate pressure vertically. This examination triggered another pain scream from the patient.
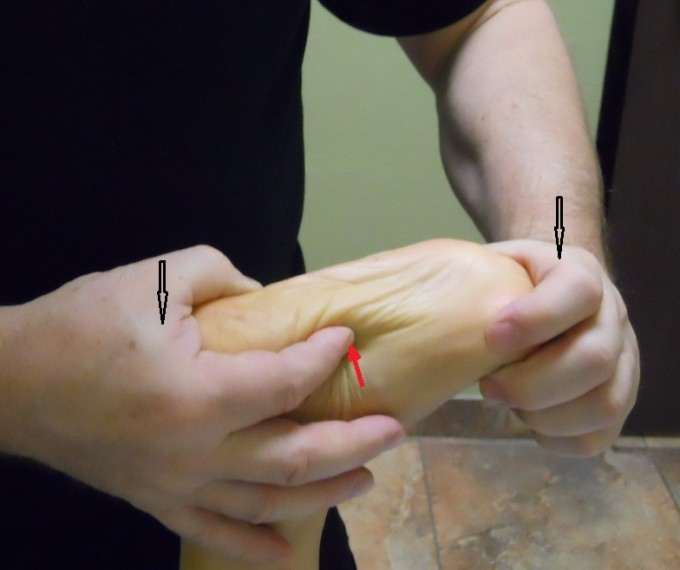
This finding means that while outer layer of the plantar fascia completely lost its elasticity the inner layer of collagen fibers still functioning. The pain which comes from the foot itself and heel is result of this inner tension.
We recommended her to stop wearing orthotics since according to the patient she felt that they hurt her feet more than helped. We asked her to buy Dr. Scholl’s gel inserts for $10, gave her set of home stretches, forbid ice application which she constantly used as recommended by her podiatrists, encourage her to do Epson salt feet baths two times per day.
In regard to the treatment protocol. We used standard protocol for Plantar Fasciitis from the Medical Massage Library but we modified it to be more effective for this particular patient. We concentrated on the part of plantar fascia just at its insertion to metatarsal heads and gradually applied the Periostal Massage on the metatarsal heads (see picture above for the direction of friction and compressions).
Another modification was work in the inner layer of the plantar fascia. We used the same trick we applied during the examination. Using tip of the index we penetrated as far as possible under the fascia from the medial edge of foot along inner foot arch and work along it.
Switch to gel inserts gave the patient relief just after the first session. We used 5 sessions of medical massage before giving her week break. We saw her today. For the first time in 4 years she got overall pain relief by approximately 70%. Next week we planed another push with 5-6 sessions to make results clinically stable.
LESSONS:
1. Pay attention but never used some one else ideas as guide. If the patient in your office it means one thing – people before you failed and don’t follow their ideas if they even have more credentials than you. Otherwise your therapy will be just another failure in line of previous failures. Find out what was done to exclude it from your examination and therapy
2. Spend time to examine area and tissues. You maybe surprised how much they changed especially if patient has chronic somatic abnormalities
3. Stop extensively recommend ice therapy in cases of chronic somatic pathologies. It is true that ice blocks pain analyzing system but it also blocks results of your therapy. Shower, hot bathes, Jacuzzi followed by passive stretching is only correct supportive therapy at home.
Ice is supposed to be used in case of acute trauma (first 24-48 hours), acute inflammation (e.g. rheumatoid arthritis), severe nerve pain (i.e., neuralgia)
Category: Blog , Medical Massage
Tags: Issue #1 2015
