
by Ross Turchaninov, MD and Boris Prilutsky, MA, LMT
Trigger Point Therapy (TPT) is perhaps one of the most controversial topics in modern massage literature. At the same time, it remains one of the cornerstones of Medical Massage and Manual Therapy. Across massage publications, we frequently encounter articles that are inconsistent with the scientific principles of massage therapy and often contradict one another. Periodically, so-called “new approaches” to Trigger Point Therapy are introduced, with authors claiming breakthroughs. However, these “discoveries” typically lack scientific validation, have not been confirmed through independent clinical testing, and are based primarily on anecdotal evidence and personal opinions. If we would like massage therapy to be recognized by modern American medicine, where it originated, we can’t act and treat using personal opinions as guidance.
Many practitioners are unaware that a TPT protocol grounded in science already exists—one that has undergone extensive clinical testing. Therefore, there is no need to reinvent the wheel. This four-part article presents a safe and clinically effective TPT protocol based on modern scientific and clinical data.
First, the goal of this publication is to share the existing body of knowledge with practitioners. The TPT has gradually emerged from the collective work of multiple authors from different Western countries, each making significant contributions to the science of manual therapy and medical massage.
Second, we will illustrate every detail of the TPT protocol in video format, so readers and viewers can fully master it without attending additional seminars or purchasing supplementary materials.
Third, we fully support innovation in the field of TPT—provided that any new development is rigorously and independently tested in clinical settings and its efficacy is confirmed. The moment a new treatment option demonstrates superiority over the current standard, we will be the first to adopt it.
Why do we insist on such rigorous standards in TPT in the treatment of hypertonic muscular abnormalities? Massage therapy is a field that offers considerable flexibility. When practitioners follow established safety guidelines (e.g., awareness of affected site and contraindications), it is generally difficult to harm a client. In the worst-case scenario, the treatment may simply lack therapeutic effect.
For example, one therapist may treat plantar fasciitis with Connective Tissue Massage, while another may use Myofascial Release for the same condition—both achieving positive outcomes. However, the improper application of TPT is fundamentally different. In this case, a practitioner, despite good intentions, may cause serious harm to the client’s health. Therefore, there can be no compromise in TPT: one either follows a scientifically developed protocol or risks causing damage.
We recognize that some practitioners have used TPT for years and have observed positive outcomes. This naturally raises the question: where does the harm arise? Below are the major negative consequences of improperly applied TPT:
- The “no pain, no gain” approach creates a negative perception of massage therapy—especially TPT—among clients who are already in pain or have low pain tolerance. In clinical practice, we repeatedly encounter patients who become resistant to treatment after prior painful experiences, anticipating further discomfort and worsening of symptoms.
- Incorrect application of TPT does not eliminate active trigger points but instead converts them into latent (“sleeping”) states. While this may create the illusion of successful treatment, latent trigger points can reactivate due to physical overload, emotional stress, or environmental factors such as temperature or barometric changes. In such cases, improper TPT transforms an acute condition into a chronic, sometimes lifelong problem.
- Excessive pressure applied to trigger points can cause significant damage to myofibrils. Repeated overuse of force leads to the deposition of glycosaminoglycans (GAGs) between damaged fibers, thereby initiating myogelosis. Myogelosis represents an irreversible degenerative change within skeletal muscle, palpable as dense nodules. These changes develop over years, often as a result of repeated reactivation of trigger points following improper treatment. Thus, practitioners who do not follow proper protocols may directly contribute to long-term structural damage to their clients’ soft tissues.
- Many trigger points are located near peripheral nerves and blood vessels. Improper TPT may result in serious injury to these vital anatomical structures.
- Incorrectly applied TPT or deep tissue pressure can also trigger dysfunction in internal organs.
These concerns are not theoretical. Numerous medical publications document serious complications resulting from excessive or improperly applied pressure during massage and TPT:
- Tachi et al. (1990) described autoimmune thyroiditis (Hashimoto’s disease) following painful cervical massage.
- Herkovitz (1992) reported median nerve injury after incorrect treatment of carpal tunnel syndrome.
- Danchink et al. (1993) documented muscle ossification requiring surgical removal after deep-tissue pressure.
- Liu (1993) described carotid artery dissection—a life-threatening complication—following neck massage.
- Mumm (1993) reported severe shingles along the C1-C8 dermatomes of the neck, upper shoulder, arm, forearm, and hand triggered by nerve irritation from strong cervical massage.
- Medvedev (1994) documented neurosensory hearing loss due to excessive pressure on the trapezius. The author concluded that the damage to both occipital nerves below the occipital ridge triggered the patient’s hearing loss.
- Geise (1998) reported damage to the posterior interosseous nerve, leading to long-term functional loss of the forearm and arm extensors.
- Trotter (1999) described hepatic hematoma after full-body and abdominal massage. It took six months and several blood transfusions for the patient to completely recover from the massage-induced liver injury.
- Jiang et al. (2020) reported lateral plantar nerve injury after massage therapy to relieve symptoms of plantar fasciitis. It took authors 2 months of treatment to restore the function of the traumatized nerve..
- Suh et al. (2022) documented severe median nerve damage in the forearm after massage therapy.
These cases represent only a small fraction of reported complications. Notably, many patients warned therapists about excessive pain during treatment, yet were reassured that such discomfort was “normal.” Tragically, when patients did not return after injury, practitioners often assumed successful outcomes and continued unsafe practices.
We hope this discussion clarifies our concerns regarding TPT and deep-pressure applications. Given the lack of consensus among practitioners and especially educators, it is essential to establish clear medical guidelines. If massage therapy is to be recognized as an integrative component of modern medicine, it must adhere to the same clinical standards. Above all, we must follow the fundamental principle established by Hippocrates: Primum non nocere—First, do no harm!
SHORT HISTORY OF TPT
Let us briefly review the historical development of Trigger Point Theory.
In 1843, German physician F. Froriep, MD, first described dense, painful areas within skeletal muscles—marking the earliest documentation of hypertonic muscular pathology, later termed trigger points.
In 1909, A. Cornelius, MD, proposed that painful nodules represent reflex responses of muscles and the CNS to trauma. He strongly advocated massage as the primary treatment to eliminate muscle spasm and restore normal function, developing what became known as Cornelius’ Massage.
Importantly, many modern approaches to TPT unknowingly rely on principles first established by Dr. Cornelius. Despite numerous claims of innovation, the core concepts of TPT have changed little since 1909.
What has evolved significantly is our understanding of underlying mechanisms. In 1921, Dr. H. Schade introduced the concept of myogelosis. In 1923, Dr. J. Mackenzie demonstrated the role of the nervous system, predicted by Dr. Cornelius, in the development of hypertonic abnormalities and introduced the concept of reflex zones in the skeletal muscles.
Subsequent contributions by Prof. A. Sherbak (Russia), A. Glezer, MD, and V. Dalicho, MD (Germany) further advanced reflex massage therapy. In the United States, Prof. I.M. Korr, DO, and Drs. J.J. Travell and D.G. Simons made major contributions to modern trigger point research.
FORMATION OF TRIGGER POINTS
There are three types of trigger points, each with distinct clinical presentations:
- Cutaneous (skin)
- Skeletal muscle
- Periosteal (periosteum). The periosteum is a thin connective tissue membrane covering bones, and into which all tendons and ligaments insert.
This article focuses on skeletal muscle trigger points. Each type—or their combination—can contribute to pain and dysfunction, and each requires a different therapeutic approach.
Until recently, there was no definitive evidence linking trigger points to abnormalities in myofibril function. Only with the advent of magnetic elastography in 2007 were scientists able to directly visualize myofibril involvement in trigger point formation. Fig. 1 illustrates the first recorded image of active TP in the trapezius muscle.
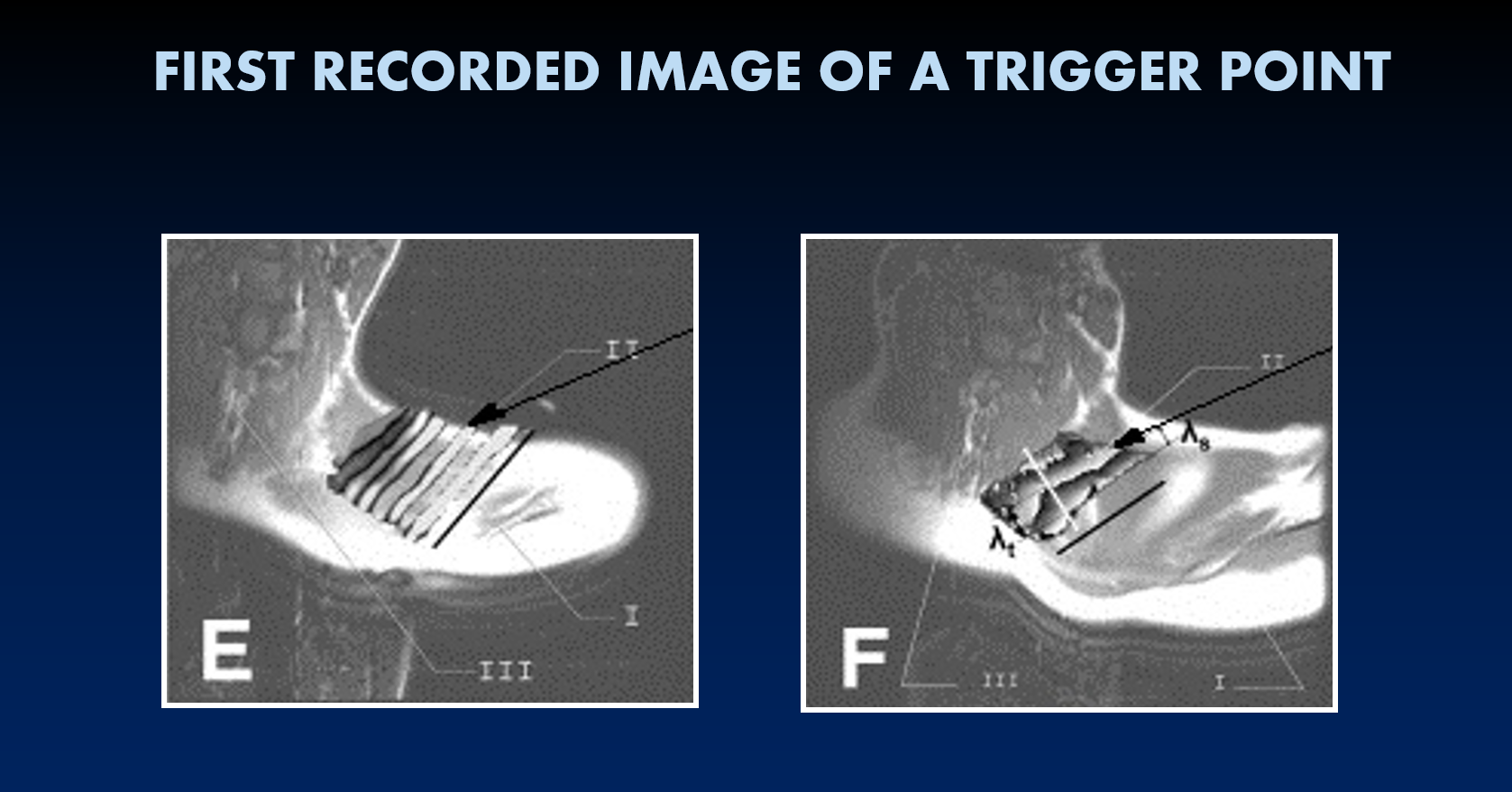
Fig. 1. Normal (E) and affected myofibrils (F) within the active TP in the trapezius muscle (Chen et al., 2007)
In the left image, you see healthy, thin myofibrils in the trapezius muscle, while in the right image, you see swollen and twisted myofibrils within active TP
During each muscle contraction, the biomechanical forces generated at the origin and insertion are directed toward each other and meet in the muscle belly. In these areas, the local circulation is inherently lower.
Additionally, neural input from the CNS to the muscle is unevenly distributed, leading to subtle twisting of muscle fibers during each contraction.
As a result of these two physiological events, the tension generated during contractions is not balanced, and the entire muscle belly becomes slightly twisted with each contraction.
It is not a problem if the muscle performs a lot of isotonic work (contraction/relaxation of the gastrocnemius muscle of a construction worker). In this scenario, the muscle pump, which supports cardiac function by pushing arterial blood into the muscle, helps to maintain proper circulation. However, the situation changes dramatically if the muscle performs many isometric, or static, contractions (as in the gastrocnemius of a bank teller). In the latter case, new waves of nerve impulses increase the muscle belly’s twists, and the muscle pump does not support cardiac work. When these events occur daily for several hours at a time (another example is a computer programmer), the affected muscle’s resting tone becomes elevated.
Resting muscle tone reflects baseline muscle tension assigned by the motor cortex. When elevated, especially during the night, it restricts arterial inflow. Clinically, this presents as morning stiffness—the earliest sign of developing muscular hypertonicity.
Before we discuss how muscle hypertonicity formed, we need to briefly review the power source used for the muscle work. Its disruption is a major factor contributing to muscle tension. Let’s use the analogy of a car engine and a muscle. The engine can’t run without gas, and muscles need ATP to contract AND relax. In the ribosomes of each myofibril, ATP is continuously synthesized from ADP, Mg, and oxygen via the process of oxidative phosphorylation. A decrease in oxygenation triggers depletion in ATP storage. All available ATP is used for contraction, and its depletion prevents the muscle from relaxing and reducing myofibrillar tension. As a result, the affected muscle is continuously spasming, with active TPT formation at its epicenters.
Now we will discuss the formation of hypertonic muscle abnormalities. It is a complex chain of events, and it will be easier to discuss it using Fig. 2.
Fig. 2. Formation of hypertonic muscular abnormalities
As a result of any, or of any combination of initial triggers, muscle hypertonicity can form (upper part of Fig. 1): trauma, chronic muscle overload owing to a lot of isometric contractions, irritation of the spinal or peripheral nerves, chronic visceral disorders, autoimmune abnormalities, nutritional deficiency, as well as some medications.
↓
The first clinical outcomes of these triggers are vasoconstriction and increased resting muscle tone. A decrease in arterial supply is also accompanied by reduced local metabolism. At this initial stage, the mismatch between the oxygen requirements of the working muscle and the circulatory system’s ability to deliver the necessary oxygen to the tissue is critical. Thus, while resting muscle tone increases and arterial blood perfusion subsequently decreases, the muscle continues to receive motor commands from the CNS to perform contractions. This mismatch becomes the initial trigger of hypertonic muscular abnormalities (Bernstein, 1947; Ivanichev, 1990).
↓
At the same time, chronic muscle tension delays venous and lymphatic drainage from the affected muscle, leading to interstitial edema (fluid accumulation between cells).
↓
All these events contribute equally to the development of local ischemia or to an inadequate arterial blood supply, and it triggers changes in local pH.
↓
Only as of this point, nociceptors (a.k.a pain receptors) are activated, and they send ascending signals to the thalamus and sensory cortex, where pain perception is formed. brain.
↓
The first outcomes of pain perception are changes in the patient’s behavior and emotional state. They start to avoid using the affected muscles and instead overload the muscle synergists. It now exacerbates a muscle imbalance, and the brain forms additional protective muscle tension, further restricting movement in the affected muscles, leading to postural changes and soft-tissue adhesions.
↓
The combination of insufficient arterial circulation, interstitial edema, local ischemia, changes in local pH, activation of the pain-analyzing system, and behavioral changes is an equally important mechanism in the development of hypertonicity and trigger points. Without proper treatment, myofibrils become swollen (see Fig. 1), and glycosaminoglycans (GAGs) are deposited between myofibrils. GAGs are compounds that consist of a large carbohydrate part and a small protein part. When deposited, GAGs slow and weaken myofibril sliding.
↓
The next pathological step is the deposit of collagen in the same area, which replaces GAGs. As a result, connective tissue forms between myofibrils, forming the core of myogelosis, a condition characterized by complete, local myofibrillar degeneration.
Tichy and Seidel (1969) showed that autoimmune mechanisms also contribute to chronic muscle hypertonicity. Autoimmune reactions are triggered in the affected muscles and connective tissues, and the immune system starts to attack the muscle tissue in the affected area, further worsening the clinical picture.
The formation of reflex zones in the skeletal muscles may also be caused by chronic visceral disorders through autonomic reflex pathways, endocrine pathology (e.g., hypothyroidism, hypoglycemia), menopause, some nutritional deficiencies (in vitamins: C, the B group, folic acid; in minerals: potassium, iron, calcium), as well as some medications (e.g., cholesterol-reducing drugs, hormone replacement therapy etc.).
In the next issue, the second part of this article will cover the diagnostic evaluation of trigger points in the skeletal muscle.
SOMI is seeking clinically oriented therapists who are willing to enter the professionally exciting field of MM to study its theory, soft-tissue evaluation, and the clinical application of MM protocols. Join SOMI for Live Webinar and Hands-on Seminars as a part of the Medical Massage Certification Program and inject clinical science into your practice! Stop wasting your time and resources on personal opinions. We will share real scientific and clinical data with you to change how you practice MT!
Here is SOMI’s 2026 schedule: Medical Massage Courses & Certification | Science of Massage Institute » Medical Massage Continuing Education
Great first step in the journey to Medical Massage practice based on science and its clinical application is SOMI’s Live Webinars on Medical Massage Theory and Soft tissue Evaluation, May 2-3:
AND
Medical Massage Techniques on May 16-17:
REFERENCES
Bernstein N.A. The Structure of Movements. Academy of Science, Moscow, 1947
Chen, Q., Bensamoun, S., Basford, J.R., Thompson, J.M., An, K.N. Identification and quantification of myofascial taut bands with magnetic resonance elastography. Arch Phys Med Rehabil. 2007; 88 1658–1661.
Cornelius A. Nervenpuncte, ihre Entstehung, bedeutung und behandlung mitters Nervemassage. Thime, Leipzig, 1909
Danchik J.J., Yochum T.R., Aspergen D.D. Myositis Ossificans Traumatica. J. Manip. Phys. Ther., 16(9);605-614, 1993
Froriep R. Ein Beitag zur Pathologie und Therapie des Rheumathismus. Weimar, 1843
Geise S. Posterior Interosseus Syndrome Resulting from Deep Tissue Massage.Plast. Reconstr. Surg, 102(5):1778-1779, 1998
Glezer O., Dalicho V.A. Segmentmassage. Leipzig, 1955
Herkovitz S. Shiatsu Massage-Induced Injury of the Median Reccurent Motor Branch. Muscle Nerve, 15(10):1215, 1992
Ivanichev G.A. Painful Muscular Hypertonus and Trigger Points. Kazan Medical University, Kazan, 1990
Jiang Z., Zhang H., Yu T., Du Y., Qian Z., Chang F. Musculoskeletal ultrasonography combined with electromyography in the diagnosis of massage-induced lateral plantar nerve injury: A case report. Medicine (Baltimore). 2020 Jul 10;99(28):e21130.
Korr, I.M. The Neural Basis of the Osteopathic Lesion. JAOA, 47(4):191-198, 1947
Liu B. Extracarnial Internal Carotid Artery Dissection Secondary to Neck Massage. Vizualization of Mural Hematoma by MRI. Kao. Hsiung I Hseeh Ko Hsuenh Tsa Chin., 9(5):332-327, 1993
Mackenzie J., Angina Pectoris. Henry, Frowde & Stroughton, London, 1923
Mikhail A, Reidy JF, Taylor PR, Scoble J.E. Renal artery embolization after back massage in a patient with aortic occlusion. Nephrol Dial Transplant 1997;12:797–8.
Medvedev E.A. Case of Acute Unilateral Neurosensory Hearing Loss Caused by Massage of Trapezius Muscle. Vest. Otorinolaringol, 3:38-39, 1994
Mumm A.N. Zoster After Massage. Lancet, 341(8842):447, 1993
Schade H. Untersuchungen in der Erkaltungstrade: III Uber den Rheumatismus, in besondere den Muskelrheumatismus (Myogelose). Munch Med Wschr 68, 95-99, 1921
Sherbak A.E. The Physiological Effect of Reflex Massage. Medgiz, Moscow, 1936
Suh M.R., Song J. H, Park Y, Lee S.H., Ahn J. Case report: Traumatic median neuropathy in the distal forearm after massage therapy. Front Neurol. 2022 Sep 21:13:959919
Tachi J., Amino N., Myai K. Massage Therapy on neck: A Contributing Factor for Destructive Thyrotoxycosis. Thyrology, 21(1):25-27, 1990
Tichy H., Seide K. Reitrage zur Rheumatologie. Berlin, 1969
Travel J.G., Rinzler S.H. The Myofascial Genesis of Pain. Postgrad. Med.,11:425-434, 1952
Travel J.G., Simmons D.G. Myofascial Pain and Dysfunction. The Trigger Point Manual. Williams&Wilkins, 1983
Trotter JF. Hepatic hematoma after deep tissue massage. N Engl J Med 1999;341:2019–20.
ABOUT THE AUTHORS

Here is a video on Dr. Ross Turchaninov’s Bio: Who is Dr. Ross Tourchaninov? – YouTube

B. Prilutsky , LMT, MA has practiced and taught Medical and Sports Massage for more than 40 years. He has a master’s degree in physical education and rehabilitation from Ukraine.
Boris has worked with athletes and world dignitaries throughout Europe, Israel, and the USA. He is the founder of the Institute of Professional Practical Therapy in Los Angeles, and to date, he has trained thousands of therapists worldwide. Boris Prilutsky has published extensively on various topics of physical medicine and rehabilitation.
Category: Medical Massage
