
by Dr. Ross Turchaninov and Boris Prilutsky, MA, LMT
In the first article, Medical Massage Courses & Certification | Science of Massage Institute » Science of Trigger Point Therapy. Part I: Nature of Trigger Points we briefly reviewed the history of the trigger point concept and the major mechanisms of trigger point formation. This part of the article examines trigger points and their differentiation.
TYPES OF TRIGGER POINTS (TP)
One of the most common mistakes practitioners make is believing that trigger points are a pathology associated only with skeletal muscles. From book to book and from article to article, authors discuss TPs in skeletal muscles and various approaches to their treatment without even mentioning that trigger points may develop in three types of soft tissue: the skin (cutaneous TPs), skeletal muscles, and the periosteum (periosteal TPs).
In many cases, practitioners do not consider these “other” TPs important or clinically valuable, simply because this essential component of massage science was never taught in massage school and is rarely mentioned in publications or educational seminars.
In real clinical practice, however, practitioners encounter clients with active TPs in all three types of soft tissue on a daily basis, often without recognizing their presence during evaluation or incorporating them into the treatment protocol. This oversight alone reduces clinical effectiveness and eventually leads to client dissatisfaction due to a lack of meaningful progress.
Although the primary focus of this article is TPs in skeletal muscles, we would like to briefly introduce TPs in the skin and periosteum. Proper differentiation between these types and skeletal muscle TPs is an essential component of successful somatic rehabilitation using Medical Massage.
Everyone involved in somatic rehabilitation should keep in mind a simple reference table (see Fig. 1), which allows practitioners—even during the initial client interview—to determine whether other types of TPs contribute to the client’s symptoms.
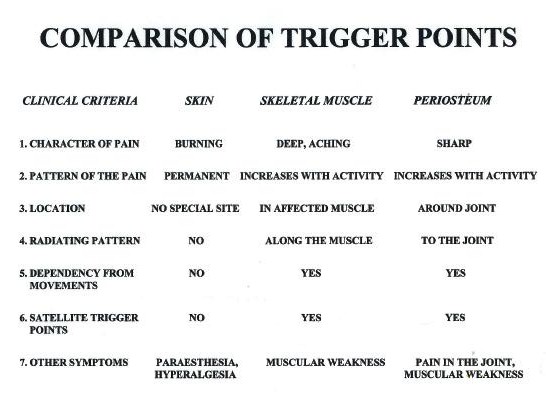
Fig. 1. Clinical differentiation of trigger points
Cutaneous Trigger Points
Cutaneous TPs were first described and extensively studied by Dr. D. C. Sinclair in 1948–1949. The primary clinical manifestation of cutaneous TPs is a combination of localized pain AND a burning sensation on the skin. Patients often describe this sensation as if a hot coin has been placed on a specific area of the body. This burning discomfort is frequently accompanied by tingling in the surrounding tissues.
The presence of cutaneous TPs always indicates underlying nerve irritation. For example, in cases of Sciatica, irritation of the sciatic nerve may lead to the development of cutaneous TPs along the leg or foot. However, a more common clinical scenario is the formation of cutaneous TPs in the upper and middle back due to irritation or compression of the cutaneous branches of the spinal nerves that innervate dermatomes in these regions.
A typical mechanism of cutaneous TP formation in the upper back involves the following chain of events: prolonged computer work requires the client to maintain a fixed head position and steady visual focus for extended periods.
⇓
This leads to excessive isometric activity of the trapezius muscle, increasing muscle tension and resting tone.
⇓
After branching from the spinal nerve, cutaneous nerves pass through multiple layers of soft tissue: the deep fascia between the trapezius and rhomboid muscles, the belly of the trapezius, and the superficial fascia covering the muscle. Only after traversing these layers do cutaneous branches reach the skin to innervate the corresponding dermatome. (See Fig. 2 for the map of dermatomes and matching cutaneous branches of the spinal nerves in the back. To see the full picture, please click on the image.)
⇓
When the soft tissues in the back are hypertonic, they compress the cutaneous branches, which triggers the development of the cutaneous TPs in the dermatomes supplied by the irritated or compressed cutaneous nerve.
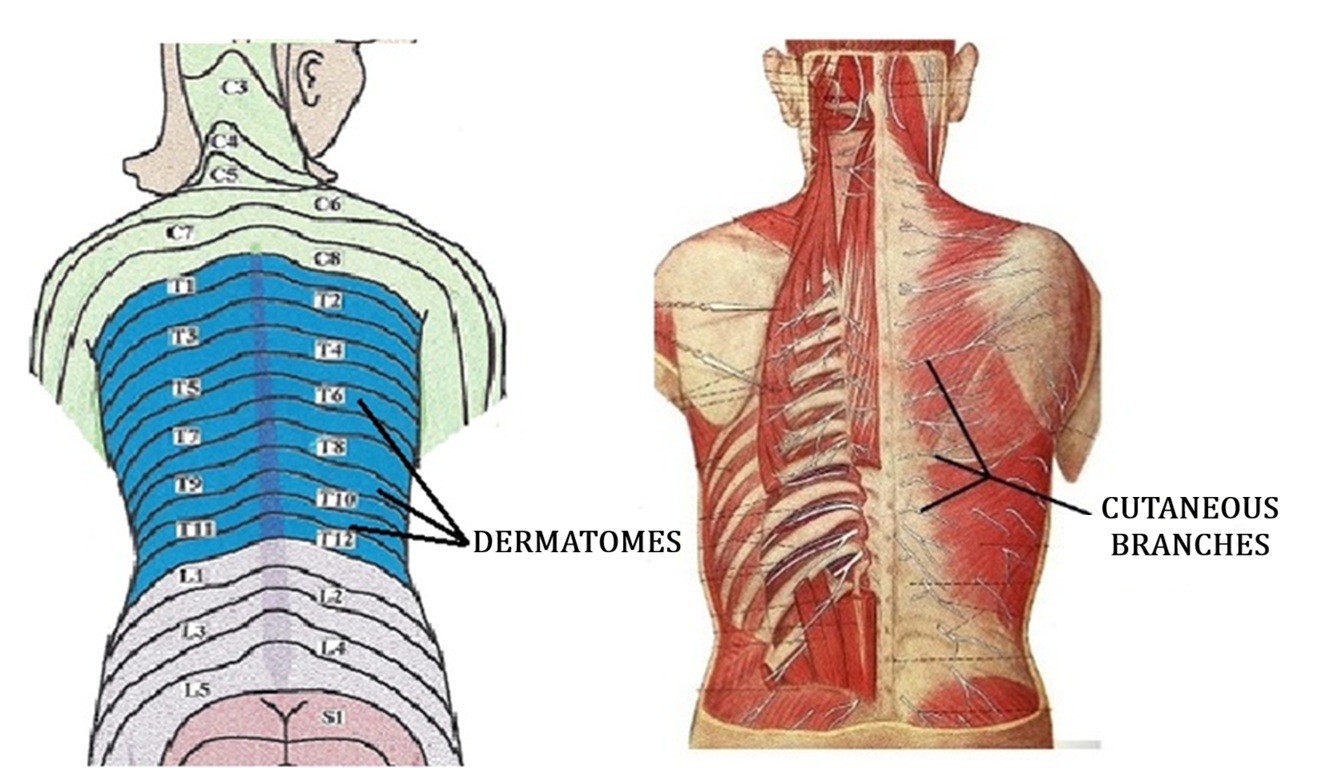
Fig. 2. Dermatomes and cutaneous branches of the spinal nerves (skin and superficial fascia removed)
Because patients experience persistent burning and tingling, they often rub the affected area. This repeated friction may lead to local skin microtrauma and subsequent pigmentation. In such cases, the active trigger point (TP) may become visibly apparent.
Figure 3 demonstrates a cutaneous TP in our patient with left middle back pain. The area of skin pigmentation precisely corresponds to the location where the patient reported a burning sensation.
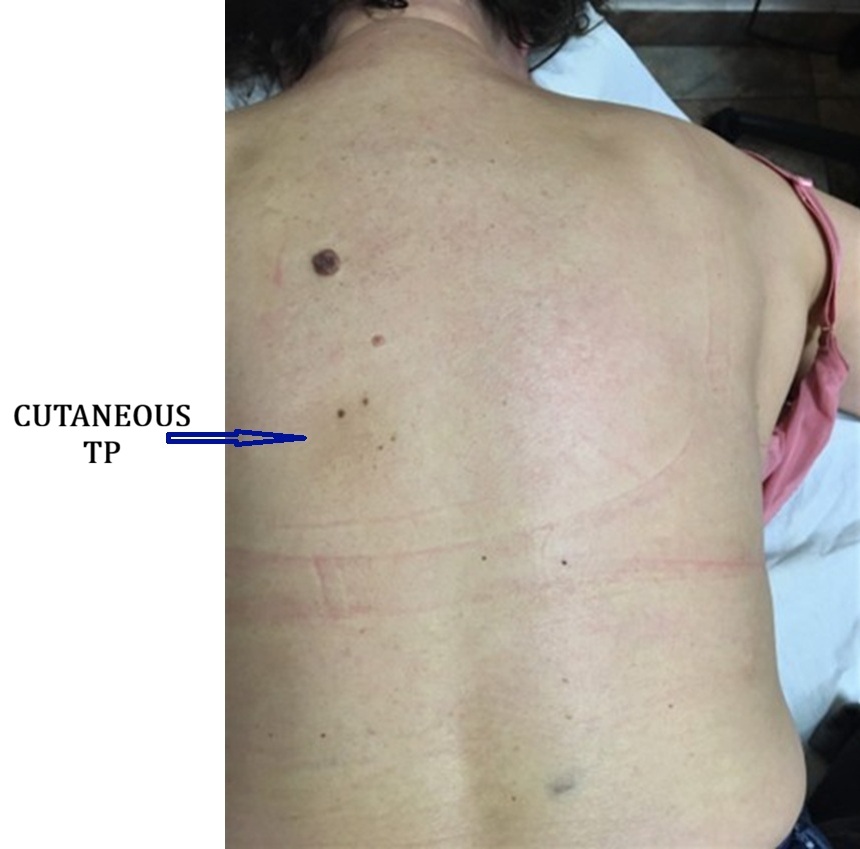
Fig. 3. Active cutaneous TP in a patient with left-sided middle back pain (To see the full picture, please click on the image).
In some cases, patients present with all clinical signs of an active TP within the skeletal muscles while simultaneously reporting a localized burning sensation. This indicates that an active cutaneous TP overlies an active muscular TP. It is important to recognize this combination, as each must be treated differently.
Periosteal Trigger Points
The concept of periosteal trigger points (TPs) and Periosteal Massage for their treatment was developed by the German physicians Paul Vogler and Herbert Krauss in the 1940s.
Periosteal TPs form within the periosteum—a dense connective tissue membrane that covers the outer surface of all bones and is firmly attached to them. The periosteum plays a critical role in bone metabolism, innervation, and fracture healing, and serves as the attachment site for tendons, ligaments, and fascia.
The periosteum is richly innervated; therefore, TPs that develop within it are extremely painful. In fact, periosteal TPs are among the most painful trigger points encountered in clinical practice. Patients with acute Tennis Elbow, Golfer’s Elbow, or De Quervain’s Disease frequently report that even minimal movement of the affected joint produces excruciating pain.
High-intensity joint pain triggered by active movement and accompanied by muscle weakness are key clinical signs of periosteal TPs (Vogler & Krauss, 1953).
CLASSIFICATION OF TRIGGER POINTS IN SKELETAL MUSCLES
A critical component of skeletal muscle evaluation is understanding the nature of trigger points (TPs) and accurately identifying their locations. Let us begin with the definition of a TP. Although the client perceives a TP as a pinpoint of pain, the actual affected area within the muscle is not circular. It is more accurately described as a spindle-shaped zone located within the muscle belly. Thus, a TP represents an epicenter of muscle hypertonicity, where numerous myofibrils exhibit maximal spasm.
This localized spasm is a fundamental factor in TP formation, as it compromises blood circulation within the affected tissues (Fassbender & Wegner, 1973; Popelansky et al., 1976; Janet Travell & David Simons, 1983).
According to the widely accepted classification (Travell & Simons, 1983), trigger points in skeletal muscles are divided into:
- Active Trigger Point (ATP)
- Latent or “Sleeping” Trigger Point (LTP)
- Satellite or Referred Trigger Point (STP)
- Secondary Trigger Point (SCTP)
- Motor Trigger Point (MTP)
1. Active Trigger Point (ATP)
Active trigger points (ATPs) are the key drivers of muscle hypertonicity and all associated symptoms in the affected area. An ATP represents the site of greatest pain, either during active movement or upon direct palpation.
ATPs typically prompt the client to seek medical help, as they serve as the epicenter of acute pain and muscle dysfunction. Pain originating from an ATP often radiates along the fibers of the same muscle or throughout the entire muscle group.
Another important clinical sign is muscle weakness. A muscle harboring an ATP may become sufficiently weakened that it cannot effectively execute motor commands from the central nervous system.
ATPs tend to localize in predictable regions within specific muscles. For this reason, TP maps are valuable diagnostic tools in clinical practice.
2. Latent or “Sleeping” Trigger Point (LTP)
A latent trigger point (LTP) is an active TP that, due to self-treatment or inadequate professional intervention, has not been eliminated but has transitioned into a “sleeping” state.
LTPs do not cause pain at rest or during typical physical activity. However, they are a major cause of muscle stiffness, especially in the morning. Muscles containing LTPs are more easily fatigued and exhibit reduced strength. Mild discomfort may also appear at the end range of movement.
LTPs can be readily reactivated into active TPs and vice versa. Clinically, they represent a chronic state of hyperirritability in muscle spindle receptors, leading to persistent muscle hypertonicity.
Reactivation of LTPs may be triggered by factors such as physical overload, postural stress, or temperature changes. The ongoing transition between latent and active states contributes significantly to the development of myogelosis. As we discussed in Part I of this article, myogelosis is an irreversible degeneration of myofibrils.
3. Satellite or Referred Trigger Point (STP)
Satellite trigger points (STPs) are also painful areas of muscular tension; however, their intensity is lower, and their size is typically smaller than ATPs. STPs contribute to overall muscle pain, weakness, and hypertonicity.
Patients usually do not perceive STPs as distinct pain sources. Instead, they experience them as the radiation pattern originating from an active TP (Jacobs, 1960; Popelansky et al., 1976; Travell & Simons, 1983).
Therefore, accurate identification of STPs requires careful assessment of the patient’s pain referral patterns and targeted examination of these regions.
4. Secondary Trigger Point (SCTP)
Muscles involved in joint movement are categorized as prime movers and synergists. The prime mover is the primary muscle responsible for a specific movement, while synergists assist when additional force is required. For example, during elbow flexion, the biceps brachii serves as the prime mover, while the brachialis and brachioradialis act as synergists.
Secondary trigger points (SCTPs) develop in synergistic muscles due to their overload. When the prime mover contains an active TP, it becomes weakened and cannot generate sufficient force. Consequently, synergists are forced to compensate and work beyond their physiological capacity. This chronic overload leads to the formation of SCTPs in the assisting muscles.
5. Motor Trigger Point (MTP)
Some authors (Gunn et al., 1976; Travell & Simons, 1983) describe motor trigger points (MTPs) at the neuromuscular junction, where the motor nerve enters the muscle.
Studies have shown that these areas produce the strongest muscle contractions in response to minimal electrical stimulation. In clinical literature, the terms “trigger points” and “motor points” are sometimes used interchangeably.
The formation of MTPs is typically a secondary response to nerve irritation caused by chronic muscle and fascial tension. Histological studies (Heine, 1997; Gogoleva, 2001) indicate that persistent low-grade inflammation around motor nerve endings leads to fibroblast activation and collagen deposition. This process forms so-called “collagen cuffs” around the neuromuscular junction.
These collagen deposits interfere with the precise neurochemical transmission between the motor nerve and muscle fibers, contributing to pain generation in the MTP region.
MTPs also hold important diagnostic value. Their widespread presence may indicate spinal nerve irritation or compression, such as from a bulging intervertebral disc (Gunn et al., 1976). This possibility should always be considered during clinical evaluation.
EVALUATION OF THE TRIGGER POINTS IN THE SKELETAL MUSCLES
As we just discussed above, there are several types of TPs in the skeletal muscles. In very complicated, long-standing cases of muscle hypertonicity, several types of TPs may coexist, which is the most confusing part of Trigger Point Therapy.
Let’s simplify the evaluation of TPs as much as possible. We will provide you with simple, effective tests and diagnostic techniques you can start using in your massage room immediately.
Evaluation of Active Trigger Points (ATP)
An active trigger point (ATP) is the most painful area within a muscle spasm. Detecting ATP at the very beginning of the evaluation is critical. This task is relatively simple when the client presents with an acute case, and only one ATP is present. The situation becomes much more challenging when the practitioner is dealing with chronic muscle hypertonicity. In such cases, satellite or motor trigger points may complicate the examination and frequently mislead the practitioner.
Early detection of the ATP is essential because it often holds the key to the entire pattern of tension in the affected area. If the practitioner makes an incorrect decision and treats a secondary trigger point instead of the ATP, he or she is fighting windmills.
How to Detect an ATP
1. Questioning
Ask the client to pinpoint the most painful area. Then ask them to demonstrate the movement that triggers the most intense pain in that area. Match this information with the map of trigger points.
2. “Jump Symptom” Test
There are only a few diagnostic tools available to evaluate hypertonic muscular abnormalities, and the “jump symptom” remains one of the most effective (Fisher, 1988). Always begin by palpating the affected area with pressure just below the pain threshold. Try to detect structural changes within the examined muscle, such as dense areas, taut bands, or localized tension. Ask the client to report any pain sensations and their intensity during the examination. Then apply pressure at the pain threshold to the suspected areas.
If the examiner contacts an ATP, the client will experience acute pain and demonstrate the so-called “jump symptom,” which is a sudden withdrawal of the examined body part, or even of the entire body, away from the practitioner’s hand (Kraft et al., 1968).
The video demonstrates the application of the Jump Test to ATPs in the trapezius muscle. At the beginning of the video, the black dot indicates the most common location of the ATP in the lower portion of the trapezius muscle. The second part of the video shows the client’s reaction to the Jump Test. All videos in this article are taken from our Video Library of Medical Massage Protocols (Medical Massage Courses & Certification | Science of Massage Institute » Welcome to the Video Library!
3. Movement Test
If the client presents with a recent case of hypertonic muscular abnormality involving a single trigger point (TP) in one muscle, diagnostic evaluation is relatively straightforward. However, the situation becomes significantly more complex in chronic cases, where there is a long history of dysfunction accompanied by widespread pain and increased muscle tension.
In such cases, applying pressure to multiple areas within the affected and neighboring muscles may elicit the “jump symptom.” As discussed earlier, the practitioner must identify and treat the active trigger point (ATP) first. The challenge arises in differentiating between multiple TPs when each produces pain of similar intensity.
The Movement Test is specifically designed for these situations. It is simple, reliable, and highly informative. By analyzing pain provoked during specific movements, the practitioner can identify the muscle that plays the primary role in generating the client’s symptoms and, therefore, locate the ATP.
The video demonstrates the Movement Test for the right shoulder. The client presents with chronic Deltoid Muscle Syndrome.
Ask the patient to perform a movement in the joint or body region that reproduces the pain (in the video, shoulder abduction). Then apply finger pressure to the examined area and ask the client to repeat the same movement.
If the practitioner is pressing on the ATP, the client will be able to repeat the movement either without pain or with only minimal, tolerable discomfort—as long as the compression is maintained (see the second part of the video). As soon as the practitioner releases the pressure and asks the client to repeat the movement, the original pain returns, and the client will again stop at the same critical level of contraction (see the third part of the video).
In other words, by applying pressure, the practitioner temporarily deactivates the ATP, providing the weakened muscle with an additional point of support. As long as ATP remains deactivated, the muscle can contract more freely.
If the practitioner applies pressure to a satellite TP rather than the ATP, the client will continue to experience pain during the movement despite maintained compression (see the fourth part of the video).
Thus, the Movement Test allows the practitioner to differentiate between various types of trigger points and quickly identify the active one.
Evaluation of Latent Trigger Points (LTP)
Clients with latent trigger points (LTPs) typically do not complain of pain or discomfort in the affected area. At most, they may report morning stiffness, which usually resolves within one to two hours.
The primary method for detecting LTPs is the “Jump Symptom” Test. When pressure is applied to an LTP, the patient demonstrates a classic withdrawal response, whereas no pain is felt without pressure. The pain disappears immediately once the pressure is released. Patients are often surprised to find pain in these areas, as they had not noticed any discomfort prior to the examination.
If LTPs are identified, they must be included in the treatment protocol and managed using the same therapeutic approach as ATPs.
Evaluation of Satellite Trigger Points (STP)
Satellite trigger points (STPs) are relatively easy to identify once the ATP has been located. The practitioner should ask the patient about any pattern of pain radiation.
If pain radiates to distant areas (e.g., from the pectoralis major to the hand), this typically indicates irritation along a peripheral nerve. However, if the pain spreads to a neighboring region within the same segment (e.g., from the anterior shoulder to the anterior chest), this pattern suggests the presence of STPs associated with the ATP.
Thus, when pain spreads within the same segment, it reflects the segmental nature of muscular hypertonicity. Pain originating from an ATP generates STPs within that same segment.
The most effective way to evaluate STPs is to apply pressure along the pathway of pain radiation identified during questioning. Typically, pressure over STPs does not provoke a strong “jump symptom,” as pain intensity is lower than that over ATPs.
It is important to identify and document the location of all STPs, as they must also be addressed during treatment.
The video below demonstrates the evaluation of STPs formed along the pathway of pain radiation from an active trigger point in the middle portion of the deltoid muscle.
The black dot represents the ATP in the deltoid muscle, while the small circle marks the muscle’s insertion on the humerus. At the beginning of the video, the patient outlines the pathway of pain radiation. In the second part, the practitioner applies pressure along this pathway and correlates it with the client’s pain response.
The final part of the video demonstrates the locations of two STPs (marked with X symbols) identified in the middle portion of the deltoid muscle.
Evaluation of Secondary Trigger Points (SCTP)
Secondary trigger points (SCTPs) are much less common compared to other types of trigger points. They typically develop from prolonged, chronic muscle tension in the prime movers.
The only reliable way to detect SCTPs is through careful palpation of the muscle synergists, where these trigger points are most often located.
A key challenge in evaluating muscle synergists is their anatomical position. They are frequently located beneath the prime mover muscles, making direct access more difficult. Therefore, the practitioner must be skilled in techniques that allow mobilization or displacement of the superficial prime mover in order to reach the underlying synergist without applying excessive pressure to the overlying tissue.
The video demonstrates the practitioner mobilizing the gastrocnemius (the prime mover) to examine a secondary trigger point (SCTP) located in the soleus (the muscle synergist). In our Video Library, we present the most common and effective techniques for mobilizing superficial muscles to access deeper muscular layers.
Evaluation of Motor Trigger Points (MTP)
Motor trigger points (MTPs) are relatively easy to evaluate. The practitioner applies direct pressure to the middle of the muscle belly—the area where the motor nerve enters the muscle and forms the neuromuscular junction. The MTP is always singular.
In muscles with short tendons, detection of the MTP is especially straightforward. The practitioner identifies the muscle’s origin and insertion, then applies vertical pressure at the midpoint between them to assess whether the MTP is active.
The video demonstrates the location of the MTP in the middle of the lateral head of the triceps brachii.
If a muscle has a long tendon, the practitioner must remember that the MTP is located in the middle of the muscle belly, not along the entire length of the muscle–tendon unit.
For example, the extensor digitorum muscle has long tendons that extend into the phalanges, while its muscle belly is relatively short. Therefore, if an MTP is present, it will be located in the center of the muscle belly rather than along the tendon.
The video demonstrates the location of the MTP in the middle of the extensor digitorum muscle belly.
Compass Technique
Let us assume that the practitioner has already identified an active trigger point (ATP) and satellite trigger points (STPs) and is ready to begin Trigger Point Therapy. However, before starting treatment, one final and critically important step remains. Without it, the therapy will be significantly less effective: the practitioner must identify the entrance into the trigger point. This can be accomplished using the Compass Technique.
As discussed earlier, a trigger point is not a flat or circular structure, but a spindle-shaped, three-dimensional area of tension within the muscle. While ATPs are located in predictable regions according to trigger-point maps, their orientation varies from case to case.
Because a TP consists of a group of myofibrils in spasm, the “entrance” into the TP corresponds to the primary direction of these contracted fibers.
Why Is the TP “Entrance” So Important?
Correct identification of the TP entrance has a direct and profound impact on the effectiveness of Trigger Point Therapy.
If the practitioner accurately determines both the location of the ATP and the direction of its entrance:
- Only minimal pressure is required to achieve effective ischemic compression
- The already compromised muscle fibers are not further traumatized
- The client does not develop protective muscle guarding
- The practitioner avoids unnecessary physical strain and fatigue
In contrast, failure to identify the correct entrance results in excessive pressure, reduced effectiveness, and increased discomfort for both the patient and the practitioner.
The widely распространенный concept of “no pain, no gain” in Trigger Point Therapy is fundamentally incorrect. It reflects a lack of understanding of these basic clinical principles.
Concept Illustration
The concept of identifying the entrance into the trigger point is illustrated in Fig. 4.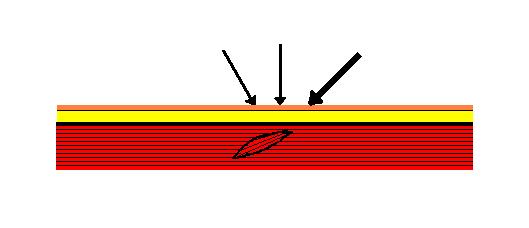
Fig. 4. Detection of the entrance into the trigger point using the Compass Technique
Tense muscle fibers that form the trigger point are arranged in a specific direction. If the practitioner applies pressure to the TP from any of the directions indicated by the thin arrows, the TP will be contacted, and the client will report acute pain accompanied by the “jump sign.”
However, when pressure is applied in the direction indicated by the thick arrow, the client experiences a distinctly different sensation—an extremely intense, often sharp or stabbing pain—despite maintaining the same level of pressure. This direction represents the “entrance” into the TP.
The practitioner should carefully note both the finger position and the angle of pressure application, as this exact direction must be used during Trigger Point Therapy to achieve maximum effectiveness with minimal force.
The video demonstrates the clinical application of the Compass Technique on the lower trapezius muscle (indicated by a black dot).
First, explain the procedure to the patient, as their active participation is essential. Place your thumb over the trigger point (TP) and slowly increase pressure until you reach the pain threshold. The patient must immediately report any pain (in the video, “Pain!”). At this stage, note the amount of pressure required to activate the pain receptors when compression is applied from this specific direction.
Once the pain threshold is reached, reduce the pressure to a light touch and slightly change the angle of the thumb. Then gradually increase the pressure again until the pain threshold is reached.
The practitioner should repeat this process—applying slow, controlled compression from different angles—until identifying the thumb position and direction of pressure that produces the most intense pain sensation at the same level of applied force (in the video, “Strong Pain!”). This specific direction represents the entrance into the TP. The practitioner must remember this angle and use it during the ischemic compression phase of Trigger Point Therapy.
For the ultimate clinical training in Medical Massage based on scientific data, join SOMI’s Live Webinars and hands-on training Seminars. Here is SOMI’s schedule for 2026:
The first important step is a live webinar on Medical Massage Theory and Soft Tissue Evaluation. Join SOMI and therapists from the around the world on May 2-3: Medical Massage Courses & Certification | Science of Massage Institute » SOMI’s MM Theory Webinar May 2-3, 2026
and
on August 1-2: Medical Massage Courses & Certification | Science of Massage Institute » SOMI’s MM Theory Webinar August 1-2, 2026
REFERENCES
Fassbender H.G., Wegner K. Morphologie und Pathogenese des Weichteilrheumatismus. Z. Rheumaforsch, 32:355-374, 1973
Fisher A.A. Documentation of Myofascial Trigger Points. Arch Phys Med Rehab, 69, 286-291, 1988
Gogoleva, E.F. New Approaches to Diagnosis and Therapy of Fibromyalgia associated with Spondylosis. Ther. Arch., 4:40-45, 2001
Gunn C.C., Milbrandt W.E. Tenderness at Motor Points. A Diagnostic and Prognostic Aid for Lower Back Injury. J. Bone JT Surg, 58-A, 6, September, 1976
Heine, H. Lehbruh der biologischen Medicine. Stuttgart, Hippokrates, 1997
Jacobs M. Massage For the Relief of pain: Anatomical and Physiological Considerations. Phys Ther Rew 40(2):93-98, 1060
Kraft G.N., Johnson E.W., LaBan M.M. The Fibrositis Syndrome. Arch Phys Med Rehab, 49, 155-162, 1968
Popelansky Y.Y., Zaslavsky E.S., Veselovsky V.P. Medico-Social Significance, Etiology, Pathogenesis and Diagnoss of Extra-Articluar Pathologies of the Extremities and Dorsum Soft Tissue. Voprosi Reumatologii, 3:38-43, 1976
Sinclar, D.C. The remote reference of pain aroused in the skin. Brain 72:364-372, 1949
Travel J.G., Simons D.G. Myofascial Pain and Dysfunction. The Trigger Point Manual. Williams&Wilkins, 1983
Vogler, P, Krauss, H, Periostbenhandlung. Leipzig, 1953
ABOUT THE AUTHORS

Here is a link to Dr. R. Turchaninov’s bio: Who is Dr. Ross Tourchaninov?

B. Prilutsky , LMT, MA has practiced and taught Medical and Sports Massage for more than 40 years. He has a master’s degree in physical education and rehabilitation from Ukraine.
Boris has worked with athletes and world dignitaries throughout Europe, Israel, and the USA. He is the founder of the Institute of Professional Practical Therapy in Los Angeles, and to date, he has trained thousands of therapists worldwide. Boris Prilutsky has published extensively on various topics of physical medicine and rehabilitation.
Category: Medical Massage
Tags: 60 Variations of 7 Basic Techniques, Journal of Massage Science 2009 #3
