
by Ross Turchaninov, MD, and Boris Prilutsky, MA, LMT
This is the third part of our article. In the first two parts, we discussed the nature of trigger points in the skeletal muscles, as well as their differentiation and evaluation.
In this part, we will discuss how Trigger Point Therapy (TPT) works and the mechanisms practitioners employ when treating hypertonic muscular abnormalities. In the final part of our article, in the upcoming issue of the Journal of Massage Science, we will discuss the step-by-step application of the TPT protocol.
Trigger point, as well as hypertonus and myogelosis, should be treated with the combination of the two approaches: direct (local) and indirect (reflex) therapy. Only in such cases does the practitioner have a chance to completely eliminate hypertonic muscle pathology, rather than suppressing it into a latent state.
THERAPEUTIC OUTCOMES OF TPT
There are three local therapeutic outcomes of TPT: stimulation of local metabolism, release of the vasoactive substances, and reflex vasodilation after the ischemic compression.
1. Stimulation of local metabolism
As we discussed before, an active trigger point is the epicenter of a local spasm, which is the leading factor in the formation of local ischemia (i.e., insufficient arterial supply) and insufficient venous and lymphatic drainage.
During the TPT, the practitioner applies soft-tissue compression that should reach the patient’s pain threshold WITHOUT surpassing it. Because of the muscle spasm, even moderate pressure will microtraumatize the capillary bed within the trigger point. When capillaries are damaged, microhemorrhages occur, and blood cells enter the soft tissue.
The body will immediately respond to the presence of free blood cells in the tissue by sending killer cells (macrophages, T cells) to eliminate them and dispose of their remains. For this process to occur, as well as a result of it, the local metabolism within the area of the trigger point must be significantly increased.
2. Release of the vasoactive substances
As discussed above, the application of direct pressure in the area of the trigger point causes mild local trauma. As a result of every trauma of the soft tissue, the vasoactive substance – histamine – is released from the tissue.
Histamine is a very potent vasodilator and the main messenger the body uses to signal fibroblasts about tissue damage. Fibroblasts are special repair cells that produce collagen, the major structural protein of all tissues and organs.
As a result of local histamine release, fibroblasts migrate into the area of the trigger point and begin collagen production. Thus, histamine release from compressed tissue further activates local metabolism, supports vasodilation, and plays a key role in tissue repair.
3. Reflex vasodilation
The trigger point is within the area of muscle spasm, where arterial perfusion is significantly reduced. The blood flow to the trigger point is still maintained to the degree needed for minimal oxygenation of the muscle tissue, but its volume is insufficient to allow the affected part of the muscle to contract and relax effectively.
However, blood flow in the area around the trigger point is not affected. During TPT, the practitioner compresses the trigger point to reduce blood perfusion through the capillaries, i.e., ischemic compression. As a result of this compression, a condition of local hypoxia (i.e., lack of oxygen) is created.
While the practitioner compresses the tissue, the patient’s heart continues to pump arterial blood, and its pressure creates a so-called ‘blood depot’ around the practitioner’s finger. As soon as the practitioner releases the pressure, the body takes extra measures to restore proper oxygenation of the compressed tissue, and fresh arterial blood from the ‘blood depot’ is immediately available.
To let this excess blood reach tissues ‘hungry’ for oxygen and eliminate hypoxia, the nervous system triggers reflex vasodilation of the constricted capillaries in the compressed area. What is more important, reserve capillaries that were not open initially, also recruited to accommodate the oxygenated blood from the ‘blood-depot’. As a result, vasospasm is eliminated, and the blood perfusion is restored.
Fig 1 illustrates thermography of the active trigger point area in the posterior shoulder. The authors of this excellent study marked the area around the active trigger point with markers and then performed thermography of the area (upper part of the image). Thermograph records even the slightest fluctuations in body temperature.
Let’s decode the thermography results on the lower part of the image. Position of markers is clearly visible. The white area indicates a lower body temperature between the markers due to local ischemia at the active trigger point.
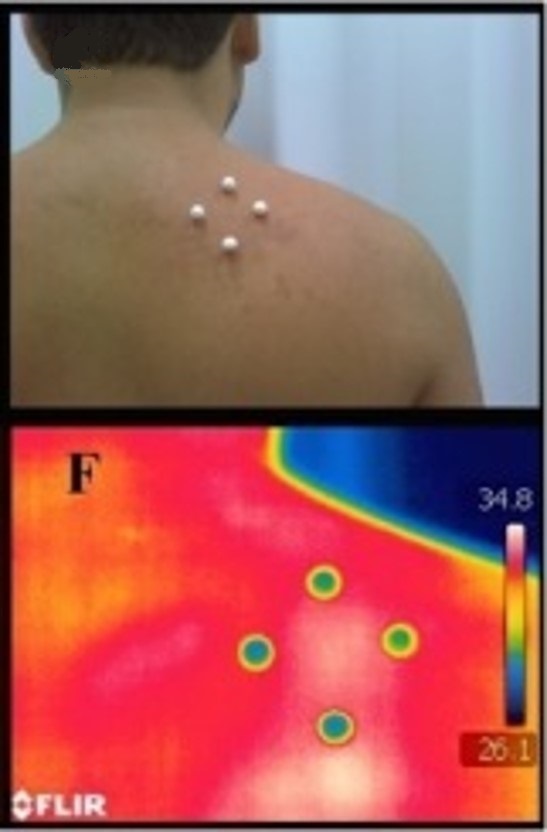
Fig. 1. Thermogram of active trigger point and blood depot (Magalhães M.F., et al., 2015)
Around the markers, the color is bright red, a visual representation of the blood depot around the active trigger point. Arterial blood, due to cardiac contractions, attempts to enter the active trigger point, but blood flow is obstructed by the local muscle spasm. Thus, the accumulation of arterial blood around the trigger point increases local temperature, which you see as bright red.
Finally, the tissues next to the bright red area are yellow. These tissues are healthy, and the local temperature is normal. The goal of correctly conducted Trigger Point Therapy is to make the entire posterior shoulder yellow in color on a thermogram by eliminating local ischemia (white area) and bright red areas (blood depot).
CORRELATION OF CONTACT AREA OF THE HAND AND TRIGGER POINT AREA
The concept of ‘blood depot’ leads to another important subject: the proper correlation between the contact area the therapist uses during Trigger Point Therapy and the trigger point itself.
The video shows two examples of TPT conducted in the biceps femoris muscle. In the first part of the video, the practitioner uses the elbow; in the second, the thumb. If one compares the contact areas of the thumb and elbow, one will see that, in the case of the elbow, the practitioner compresses the trigger point and the surrounding unaffected tissue. When the tip of the thumb is used, the ischemic compression closely matches the size of the trigger point.
Why is it so important that the contact area matches the trigger point area as closely as possible? Part 1 of the video below shows the trigger point in the biceps femoris muscle (black dot), and Part 2 shows trigger point compression using the elbow. The circular line with solid arrows in Part 3 represents the border of the ‘blood-depot’ formed around the elbow.
Part 4 of the video shows the same trigger point compressed by the thumb. In Part 5, the smaller solid circle with dashed arrows represents the border of the ‘blood-depot’ formed around the thumb.
In Part 6 of the video, the operator indicates that arterial blood from the ‘blood-depot’ needs to travel a certain distance before it enters the trigger point if the practitioner uses the elbow. This additional distance slows blood flow and diminishes the initial impact of reflex vasodilation. Thus, reflex vasodilation occurs later and persists for a shorter time.
Conversely, the small solid circle around the trigger point (i.e., compression with the thumb) indicates that the distance the blood must travel from the ‘blood-depot’ to enter the trigger point is much shorter. In such cases, at the moment of the compression’s release, blood from the ‘blood-depot’ around the thumb flows directly into the trigger point, producing stronger and longer vasodilation.
The following question is frequently asked: How will I maintain efficient ischemic compression if this patient has a large, powerful layer of skeletal muscles? In such cases, the ‘elbow approach’ seems the only possible option. However, we would like to remind the readers of the clinical value of the Compass Technique, which we discussed in the second part of this article (Medical Massage Courses & Certification | Science of Massage Institute » Science of Trigger Point Therapy. Part 2: Types of Trigger Points and Their Evaluation).
The Compass Technique provides the practitioner with very important clinical information about the ‘entrance’ into the trigger point.
If the practitioner detects the entrance into the trigger point during diagnostic evaluation of the muscles using the Compass Technique and uses this exact direction during ischemic compression, there is no need to apply excessive pressure to achieve efficient compression.
If the practitioner is at the entrance of the trigger point, the pressure during ischemic compression should be reduced, as the patient will feel severe pain, generate protective muscle tension, and fight against the therapist’s effort. Thus, the Compass technique helps the practitioner to conserve energy and prevent possible injury while avoiding the unnecessary trauma of the soft tissue, which is a very frequent outcome of inappropriate application of the TPT and formation of myogelosis.
AXON REFLEX
Another less-known mechanism responsible for reflex vasodilation is the axon reflex, originally described in 1941 (LeRoy 1941; Jacobs 1960). This is important information rarely mentioned in medical and massage publications, but it has great practical value.
Let’s start with the role of the central nervous system in peripheral vasodilation (i.e., increased blood perfusion). The peripheral sensory receptors in the area of the active trigger point have a very low threshold of activation. As soon as the practitioner places their hands on the affected area, the patient’s body will respond with local reflex vasoconstriction in all organs and tissues innervated by the segment of the spinal cord that innervates the trigger point. This is a body’s normal protective reaction.
If the practitioner continues to apply massage strokes in the affected area and uses the correct massage protocol, the spinal cord will recognize that the activation of sensory receptors in the affected area is harmless, and the spinal cord will cease motor response (i.e., signals to trigger the vasoconstriction) with the following local vasodilation in the affected area.
To reinforce peripheral vasodilation, the body employs the axon reflex, an important mechanism that the practitioner uses to increase and maintain local vasodilation. Let’s review the mechanism of the axon reflex with the help of the interactive diagram presented below. First, we will indicate the major anatomical components presented on the diagram.
To start the interactive diagram, please click the play button below. To replay the diagram, please click at the beginning of the sliding bar (blue line) located just below the diagram.
The solid vertical arrow indicates the direction of massage strokes.
A – Indicates the skin
B – Indicates subcutaneous fat
C – Indicates the subcutaneous fascia
D – Indicates the superficial skeletal muscles
E – Indicates the loop of the axon reflex
F – Indicates the ascending sensory fibers from the peripheral receptors to the spinal cord
G – Indicates the posterior horn of the spinal cord, which processes sensory information arriving from the peripheral receptors
H – Indicates the anterior horn of the spinal cord, which controls the motor response to the tissue and organs
I – Indicates the descending motor fibers from the spinal cord to the soft tissue
Blue dot – Indicates sensory stimuli that travel to the spinal cord
White dot – indicates the nerve impulses which travel inside the spinal cord between the sensory center in the posterior horn and the motor center in the anterior horn
Red dot – Indicates vasodilatory response from the spinal cord to the soft tissue
Green dot – Indicates the pathway of the vasodilatory impulses that travel to the soft tissue using the loop of the axon reflex
Now, let us put the chain of events into motion. When the sensory receptors are activated by massage strokes, they send signals to the central nervous system (moving blue dot) using the ascending sensory fibers of the peripheral nerve (letter F on the diagram). While sensory information travels from peripheral receptors to the spinal cord, a portion of the nerve fibers forms the so-called axon reflex arc (letter E on the diagram), using short collateral nerve branches to the capillaries of the tissue where the activated peripheral receptors are located. When these stimuli (moving green dot) reach the local capillary network using the axon reflex pathway, they trigger peripheral vasodilation BEFORE vasodilation stimuli from the anterior horns of the spinal cord (moving red dot) are able to reach the soft tissue in the massaged area.
Thus, the short and quick operating nerve fibers, which form the axon reflex, are responsible for the additional vasodilation in the massaged soft tissue. Interestingly, the axon reflex also plays a significant role in the long-lasting vasodilation that persists in the affected area after the client has left the massage therapy room.
TPT AND CENTRAL NERVOUS SYSTEM
To conduct TPT correctly, the practitioner must consider and understand the importance of preparation for the ischemic compression:
1. Entrance into TP must be established using Compass Techniques, as we discussed in Part II of this article
2. The affected area must be prepared using the massage in the inhibitory regime.
3. The high-frequency (60 Hz minimum) electric vibration in the form of oscillations, not percussions, has to block the pain-analyzing system before and during the application of ischemic compression,
4. Central Control Trigger must be activated
5. The contact area of the hand has to match the area of the trigger point.
To fully understand and correctly use all aspects of ischemic compression preparation, we should quickly discuss the relationship between the pain analysis system and TPT.
Control of the pain-analyzing system during the ischemic compression part of TPT is an extremely important subject, because inappropriate application of the pressure without the practitioner paying attention to the patient’s pain-analyzing system has many negative outcomes, which can destroy the therapist’s efforts and transfer active TP into a latent state, with its reactivation in the future.
Thus, applying the correct amount of pressure and controlling the patient’s pain analysis system are two critical elements of TPT. The “no pain, no gain” approach to TPT, which is frequently advocated, is a grave mistake that practitioners frequently make when addressing hypertonic muscle abnormalities.
The entire TPT protocol has one goal: to mislead the patient’s central nervous system and prevent the generation of protective muscle tension during ischemic compression, to effectively eliminate the trigger point. Thus, the practitioner must do everything in his power to conceal the application of ischemic compression to the patient’s central nervous system, which is on a 24-hour alert, guarding the affected area. The recommendation to simply press and hold the trigger point has nothing to do with real massage science.
The scientifically based protocol of TPT requires at least a basic understanding of the following concepts of the nervous system: desensitization of peripheral receptors, activation of the central control trigger, and closure of sensory gates in the spinal cord segment(s) responsible for the innervation of TP area.
All of these elements were developed by Prof. Mezlack and Prof. Wall, who are the fathers of the ‘Gate-control’ theory of pain, and their work was one of the greatest medical breakthroughs of the 20th century.
As readers know, there are two equally important parts of the pain-analyzing system: fast pain (evolutionary younger) and slow pain (evolutionary older). The fast pain analyzing system is activated as soon as the body is exposed to very strong and damaging stimuli. One does not discuss whether to withdraw the hand from a hot stove. It happens very quickly on the level of the spinal cord without conscious decision by the brain. A fast pain-analyzing system is responsible for conducting acute (noxious) pain stimuli from any part of the body, including the area of the active trigger point.
The slow pain analyzing system is responsible for the conductance of low-grade chronic pain from any part of the body. For example, the chronic somatic pain in cases of Fibromyalgia is conducted through the slow pain-analyzing system.
We discussed the Gate Control Theory of Pain and its very important role in clinical application of MM in this article: Medical Massage Courses & Certification | Science of Massage Institute » HOW MASSAGE THERAPY HEALS THE BODY. PART IV
If the practitioner applies TPT without control, the pain-analyzing system therapist activates the fast pain analyzing system, and the patient’s central nervous system immediately generates protective muscle tension. The protective muscle tension will exacerbate preexisting circulatory abnormalities and spasm, rendering all the practitioner’s efforts futile.
Desensitization of the Peripheral Receptors
To switch the fast pain-analyzing system to slow, the practitioner must desensitize the peripheral receptors (first and foremost nociceptors, a.k.a. pain receptors), a first critical step in TPT. This process is frequently referred to as the elimination of hyperirritability of the peripheral receptors.
The best way to accomplish this is to apply massage strokes in the inhibitory regime (Ivanichev, 1990; Goldberg et al., 1992) on the entire segment where the active trigger point(s) are located. The inhibitory regime requires applying the same massage strokes, in the same direction, at the same speed, and pressure. The practitioner should mostly use the kneading or a combination of effleurage (30%) and kneading (70%). Direct all strokes along the lymph and venous drainage. Usually, 1-2 minutes of preparation is enough.
Steady Application of True Electric Vibration
Prof. Melzak and Prof. Wall further extended the classical study by Dr. Zotterman (1939) and proved clinically that true electrical vibration at 60 Hz or higher is a very powerful clinical tool for desensitizing the CNS by inhibiting peripheral receptors. The massager must be placed in the area of active TP, in the direction of its entrance, and held steadily for approximately 1 minute.
Central Control Trigger
The final concept we need to address is the central control trigger (CCT). Prof Mezlack and Prof Wall were aware of the cases where seriously wounded people were able to function without even a trace of pain, despite the intensity of the somatic and even visceral trauma. Both scientists were sure that there is a mechanism inside the CNS that blocks the cortex from being bombarded by pain stimuli, despite the fact that the nociceptors continue to send massive sensory input to the brain. They called this hypothetical mechanism CCT.
Prof. Mezlack and Prof Wall examined different parts of the CNS as potential candidates for the CCT. Finally, they experimentally demonstrated that the posterior columns of the spinal cord indeed act as CCT. These sensory highways transmit information from the brain to the spinal cord segments at high speed. If information generated in the brain arrives just a fraction of a second before the actual trauma gates in the segments of the spinal cord are closed, the hypothalamus, the brain’s major control center, and the thalamus will refuse to accept pain-generating signals from the damaged part of the body. As a result, the injured person will be able to act, despite the severe trauma.
How can the practitioner activate the CCT and use it as an additional tool to control the patient’s pain-analyzing system during the TPT? The solution is very simple. During the application of the inhibitory regime and electric vibration, the practitioner should engage the patient in an active conversation on an interesting subject. Don’t let the conversation die. Consider new questions or remarks as the patient answers the previous ones. Of course, this practical recommendation is difficult to apply while the practitioner is working with the new patient, but it is worth learning about the patient’s interests, work, hobbies, etc., to use this data to better control the pain-analyzing system.
In the next part of this article, we will present the step-by-step application of Trigger Point Therapy according to clinical science.
For the ultimate clinical training in Medical Massage based on scientific data, join SOMI’s Live Webinars and hands-on training Seminars. Here is SOMI’s schedule for 2026:
REFERENCES
Golberg, J., Sullivan, S.J., Seaborne, D. E. The Effect of Two Intensities of Massage on H-Reflex Amplitude. Phys. Ther., 72(6), June, 449-457, 1992
Jacobs, M. Massage for the Relief of Pain: Anatomical and Physiological Considerations. Phys. Ther. Rew., 40(2): 93-98, 1960
Ivanichev, G.A. Painful Muscular Hypertonus and Trigger Points. Kazan Medical University, Kazan, 1990
LeRoy, R. La vie du Tissue Conjonctive et sa Defence par le Massage. Rev. De Me. Paris, 58, 212, 1941
Magalhães MF, et al., Evolution of Skin Temperature after the Application of Compressive Forces on Tendon, Muscle and Myofascial Trigger Point. PLoS One. 2015; 10(6) e0129034.
Mezlack, R., Wall, P. Pain Mechanism: A New Theory. Science, 150 (Nov): 971-979, 1956
Zotterman, Y. Touch, Pain and Tickling: an Electrophysiological Investigation on Cutaneous Sensory Nerves. J. Physiology, 95:1-28, 1939
ABOUT THE AUTHORS

For Dr. R. Turchaninov’s bio, please click here: Who is Dr. Ross Tourchaninov?

Mr. B. Prilutsky has practiced and taught Medical and Sports Massage for more than 30 years. He has a master’s degree in physical education and rehabilitation from Ukraine.
Mr. Prilutsky has worked with athletes and world dignitaries throughout Europe, Israel, and the USA. He is the founder of the Institute of Professional Practical Therapy in Los Angeles, and to date, he has trained thousands of therapists worldwide. Boris Prilutsky has published extensively on various topics of physical medicine and rehabilitation.
Category: Medical Massage
Tags: 60 Variations of 7 Basic Techniques, Journal of Massage Science 2009 #4
