
The purpose of this section of the Journal of Massage Science to inform the practitioners about valuable articles that frequently go unnoticed, as well as to point to those authors and publications who exhibit low educational standards. We do not play politics and we are not associated with any publishing company or professional association. We are a completely independent voice and we promise you direct unbiased reviews based strictly on the science.
If the author of the reviewed article does not agree with our opinion, we will be more than happy to publish his or her response and have a productive discussion over the article’s subject.
At the end of the year we will recognize and reward the author of the most important publication(s) and point to the authors of the most unscientific publication(s). We hope this will help to raise the bar of published materials in massage journals for the benefit of the entire profession.
Our Editorial Board would like to introduce the Appreciation Award for the American massage publication which has contributed the most important articles to the science of massage therapy in 2009.
The trophy is made from polished brass on a marble pedestal with an exotic wood foundation and decorated with blue agate. Its dimensions: 10 x 8.8 x 8.8″ (25 x 22 x 22 cm).

Massage & Bodywork

Somatic Research. A Map of Scientific Activity. Massage & Bodywork, Nov-Dec., pp. 122-127, 2009, by R.S.Travillian
Excellent and very smart article! We really appreciated the authors’s intellectual capacity as well as Massage&Bodywork publication of this article. We would like to mention one aspect of this article in case the readers have missed it or they don’t subscribed to this Massage&Bodywork Journal.
We know that genetic medicine recently made incredible advances, and we are on the brink of absolutely breathtaking possibilities in curing many debilitating and frequently fatal diseases. On the first look it seems that massage therapy doesn’t fit into the concept of genetic medicine and they will simply coexist in future society.
However, in reality the massage therapy may have an incredible future, even in this exciting new branch of the medicine. One of the biggest problems for genetic medicine is to find a way to deliver healthy genetic material into the cells of tissue or inner organs affected by the disease. As soon as we are able to pass this barrier the ‘new’ genetic material will be able to restore the pathologically changed cells and normalize function of the tissue or organ.
The scientists in many countries deal with transportation problem and in many cases are unsuccessful. The author of the reviewed article cited the paper published in Molecular Therapy (2004) where the authors reported that massage of the liver enhances gene transfer into the liver cells. Based on this and other articles on the same subject we think that massage therapy will find its respected place even in future medicine which more than likely will be based on gene therapy. This is only one great aspect of the reviewed article.
Myofascial Techniques. Glenohumeral Joint. Frozen Shoulder. Part I.Massage & Bodywork, Nov-Dec., pp. 118-121, 2009, by Til Luchau
What we liked about this article is the correct presentation of helpful techniques to release the pressure in the shoulder joint. However, the readers may get the wrong impression that application of two techniques advocated in the article is enough to help the patients with FS.
Unfortunately this is not the case. To eliminate the condition of Frozen Shoulder (FS) the practitioner must address the origin of the problem (there are many potential causes of FS) and combine it with therapy concentrated on the FS itself. However, it is unfair to make any final judgements, because, according to the author, it is only first part of the article.
Pathology Perspectives. CREST Syndrome. Massage & Bodywork, Nov-Dec., pp. 107-111, 2009, by Ruth Werner
The author continues to inform and educate readers on the pathology issues and she deserves a lot of credit for doing that. Her articles are among the few who raised new topics beyond the common issues of Tennis Elbow or TMJ Dysfunction. Besides the importance of these new topics for the entire profession the author writes her articles in an easy to follow format, which enhances the understanding of the pathology of complex disorders.
Essential Skills. Active Isolated Stretching. Massage & Bodywork, Nov-Dec., pp. 100-105, 2009, by Ben Bengamin and Jeffery P. Haggquist
Overall this is a good article which emphasizes the importance of stretching as a part of the treatment. Parts of it can be argued with and the cited research the authors have relied on is information published by the author of the isolated stretching.
For example the reviewed article constantly mentioned the accumulation of the lactic acid as a major reason for the muscle soreness. It seems that authors unaware about modern information on this subject. As we know now, lactic acid is not the source of the problem but rather the part of the solution the body tries to use to deal with muscle soreness. Our author O. Bouimer, LMT partly reviewed this scientific information in September-October issue of our Journal.
Functional Anatomy. The Psoas. Massage & Bodywork, Nov-Dec., pp. 95-96, 2009, by Christy Cael
Finally at least something at least partly right in the articles published by the author. The palpation of the psoas muscle is presented correctly. However, even on such an obvious topic, the author was able to miss important information which is directly connected to the subject of the article. The article shows the palpation of the psoas muscle only in the abdomen and did not even mentioned three other equally important areas which the practitioner must examine for the complete evaluation of the iliopsoas muscle. Otherwise the palpation becomes useless.
First of all it was a great surprise to find out that the psoas muscle must be examined alone. We have never encountered such a recommendation in medical or massage literature. Yes, anatomically the psoas muscle and iliacus muscle have different origins but they share the same tendon and the same point of the insertion into the lesser trochanter. This is why the psoas muscle must never be examined independently, only in the abdominal cavity (as suggested in the article) but always as one myotatic unit called iliopsoas muscle. In the article the author didn’t even mention the fact of the existence of such muscle in the human body. We can’t believe we are even discussing this subject.
The video below shows the palpation of the psoas muscle from the article and three more areas where iliopsoas must be examined: above the inguinal ligament, below the inguinal ligament and iliacus muscle in the iliac fossa. The last three areas which weren’t even mentioned in the article are even more important because there the iliopsoas muscle can be reached there directly while during the abdominal palpation the practitioner examines it through the loops of the small and large intestine.
In the video the solid line indicates inguinal ligament, the dashed line indicate the femoral artery. To palpate the iliopsoas muscle above the inguinal ligament place the fingertips just above the ligament and ask the client to lift lower extremity without bending the knee.
To palpate the iliopsoas muscle below the inguinal ligament find the pulsation of the femoral artery first (dotted line in the video), move fingertips of 2nd-5th fingers laterally from this line, apply vertical compression and ask the client to lift lower extremity again.
To palpate the iliacus muscle, position the client of the opposite side with knee and hip joint bent, gently rock his or her body to move the loops of small and large intestine to the opposite side of the abdomen and palpate the muscle in the iliac fossa as it is shown in the video.
Dimensions of Holistic Massage. Beyond Nuts and Bolts of Swedish.Massage & Bodywork, Nov-Dec., pp. 62-69, 2009, by Linda G. Means
This is a very well written article on the emotional and spiritual aspects of Swedish Massage. It definitely will be helpful for new practitioners fresh from massage school. Unfortunately, there are several trivial generalizations in the article. For example: “A Swedish massage session can be designed to clear energy blockages and induce a strong flow of energy”.
We think that the author owns to the massage practitioners a more detailed explanation of the nature of the energy she tries to clear. We would like to send the reader to an article on this subject ‘How Massage Therapy Heals the Body’ in this issue of our Journal. Overall the next article in the same journal is much more important and greatly written.
Is Swedish Massage Dead? Massage & Bodywork, Nov-Dec., pp. 36-45, 2009, by Anne Williams
What a great article! Thanks to the author and to Massage&Bodywork for the publication of this great piece. The article addresses a very sad tendency which we see more and more among massage practitioners – the disrespect to Swedish massage and the great degradation of its technical arsenal. It becomes less fashionable among the massage practitioners to offer ‘just Swedish’ and the great number of educators immediately offer their own breakthroughs which, very frequently, is complete nonsense. As a result we have ‘Dancing Elbow’ or ‘No Thumb Therapy’ and these attempts to make a quick buck undermine the entire profession.
At the same time we have a problem in the schools where Swedish massage frequently isn’t taught correctly and the absence of a unified view on its teaching and practice additionally confuses the practitioners.
The author raises her voice in this very well written and well argued article, and we would like to add our support as well. If you decide to learn new modality be sure that you fully mastermind the great technical potential of Swedish before you move further. This is your bread and butter and the foundation for success. By the way, do you know that the Swedish massage includes twelve(!) variations of kneading technique? Please before you decided to enroll in ‘No Thumb Therapy’ seminar learn all twelve variations of kneading and correct Body Mechanics to execute each one of them effortlessly. Incorporate them into your sessions and observe the response of your clients. You will see your practice grow quickly.
The same suggestion we have for those massage practitioners who sacrifice the Swedish massage for the Oriental types of bodywork. It is not that Swedish massage is “fluff and bluff’ compare to Oriental bodywork it is the practitioners’ “fluff and bluff’ education and practice.
Ironically, the scientifically based Swedish massage has more healing potential because it restores normal electrophysiology in the soft tissue (see article ‘How Massage Therapy Heals the Body’ in this issue of our Journal). However to do so the therapist must practice the Swedish massage correctly (again see the same article). Unfortunately, in many cases, the practitioners don’t use even a fraction of the healing power of the Swedish massage in their everyday practice.
The author is correct in that we at least partly have to thank NCBTMB for that. NCBTMB doesn’t certify practitioners in massage therapy anymore. Unfortunately the national certification at this point is fragmented certification in different modalities and in the Oriental bodywork which is frequently based on 5000 years old figurative language and concepts.
We are not so enthusiastic as the author about potential revival of the science-based Swedish massage in the near future, but it is great that this conversation even got started.
Thank you Anne Williams and Massage&Bodywork!
Massage Therapy Journal
Body Mechanics. Joint Mobilization of the Low Back. Massage Therapy Journal 48(4):97-98 winter 2009, by Joe Muscolino, DC
A great article on joint mobilization in the lower back. We really like Dr. Muscolino’s column, because it consistently provides high quality professional information and it is a great educational source.
The topic of the article and its presentation are great but it can be challenging if the practitioner has decided to use it inappropriately on the clients with pathological changes in the disc. This issue is emphasized on the first page of the article, but we would like to be sure that the readers did not miss this important piece of information.
Research Literacy. Speaking the Same Language. Massage Therapy Journal48(4):93-95 winter 2009, by Martha Brown Menard, PhD, CMT
In this issue we address the communication problem the massage practitioners have when they try to explain their services to other health practitioners. This article touches the same problem but from the different perspective. The article provides the practitioners with list of major on-line sources which are a great tool for the practitioners to educate themselves and be able to effectively communicate with other health practitioners to build up a thriving practice. Please pay attention to this important list.
Massage Today
The Silent Progression of Kidney Infections and Stone Formation.Massage Today, 9(11):21, 2009, by Dale Alexander, PhD, LMT
The article correctly raises awareness of the practitioners to the fact that chronic kidney abnormalities in the majority of cases are associated with lower back tension and pain. As a matter of fact the formation of the reflex zones in the skin, fascia, muscles and periosteum of the lower back is one of the important factors responsible for the further progression of the original kidney disorder.
The article is correct when it emphasizes the importance of asking correct questions and to consider the kidney abnormality especially in cases when lower back pain and tension greatly resists the treatment protocol.
An Alternative Approach to Stretching. Massage Today, 9(11):16, 2009, by Whitney Lowe, LMT
Excellent article! In the short one page piece the author was able to touch upon many important subjects, educate the readers and show his deep understanding of the subject. We were also very pleased by the following passage:
“There is a variety of active assisted techniques and they go by different names as PIF, muscle energy technique, active isolated stretching or facilitated stretching. There are slight variations in each of these methods, but they are all based on the neurological principles of post-isometric relaxation (PIR) and reciprocal practitioner”.
Unfortunately, the massage practitioners are bombarded with so called ‘new’ types of stretching by the educators who use an already existed method, slightly change it (frequently making it less effective as a result), give it new name and try to sell it as a new breakthrough. We greatly appreciate the author’s courage to stand up for the real science.
Fixing Achy Hips. Massage Today, 9(11):10; 22, 2009, by Erik Dalton, PhD
A good and diagnostically important article which addresses the very frequently overlooked factor of lower back pain and tension – the pelvic rotation as a result of foot positioning and incorrect dynamic of the femoral head.
The article establishes a clear pathophysiological link between these factors which the practitioners need to consider during the client’s evaluation and formulation for correct MEDICAL MASSAGE PROTOCOL.
Rheumatoid Arthritis. Massage Today, V. 9(12), 2009, by Elaine Stillerman, LMT
A good article which gives practitioners the basic overview of RA and the treatment options the modern medicine offers to these patients. The article is written from a personal perspective because the author herself suffers from RA. Definitely the article reflects the author’s personal experience with the different treatments of this very complex abnormality.
The most important part of the article is its final section where it is obvious that there is no one modality or the treatment method which helps to control RA. The only way the patients with RA are able to succeed is through the combination of therapies, or what we now call integrative medicine.
Massage
The Feldenkrais Method. Move To Improve. Massage 162, Nov:54-57, 2009, by Nancy Wozny
A good article for those practitioners who are not familiar with Feldenkrais Method and would like to learn for themselves or to teach their clients. What we like about the article is that the author emphasizes the importance of self-care aspect of it for the practitioners to relieve stress and tension accumulated as a result of work. The Feldenkrais Method is a great way to do that.

Expert Advice. What is Connective Tissue Massage? Massage 162, Nov:54-57, 2009, by John Latz
Overall this is a good article which gives the general review of the connective tissue structure, function and basic principles of connective tissue massage. What troubles us is a grave mistake we see from articles to articles published on various subjects in massage literature. This mistake is fragmentation of the profession. Without any doubt these articles split our great profession into a countless number of modalities which very frequently placed by their authors conflict with each other. This fragmentation kills the profession in the eyes of clients and what is equally important in the eyes of other health practitioners. Some passages in this article do exactly that. To quote:
“Having practiced fascial manipulation for 25 years, my hands do not readily remember how to massage muscles”
and
“Proper technique for working with muscles will not change the fascia. Understanding this ensures I am either working on the muscle or fascia, but not attempting to work with both at the same time”
During this year we reviewed a lot of articles with, let’s say, questionable para-scientific statements. These two are among the most bizarre ones! These quotes not only contradict even basics of anatomy and physiology they kill whole idea of an integrative approach to the somatic rehabilitation. This idea is the cornerstone of the entire massage therapy profession but apparently the author is not familiar with it.
As the article correctly mentioned the ‘…fascia surrounds the muscles … as the fascial envelope (myofasia)”. Fascia very tightly attached to the muscles and collagen fibers in the fascia have the predominant orientation in the direction of the muscle fibers. This why the fascia and muscle, despite the anatomical and histological differences in the structure, form the same biomechanical unit. To separation of them on the basis of the pathological changes or treatment shows deep misunderstanding of this subject.
The article correctly states that shortened fascia restricts muscle contraction and function, which in turn causes pain and tension. The sad fact is that the article tells readers only half the story. There is no way fascia and the muscle it covers can be separated and the pathological chain of event may go in the opposite direction.
Let’s look at the very frequent scenario. If skeletal muscle harbors active trigger point the shortening of the fascia develops secondarily. In such case addressing the fascia alone using connective tissue massage only without elimination of the active trigger point and restoration of the anatomical length of the tensed muscle will never take care of the origin of the problem. This is a waste of effort because the spastic muscle will shorten the fascia again.
The best outcome of such treatment is transferring active trigger point into the ‘sleeping’ or latent state instead of its complete elimination. Such insufficient therapy, i.e., application of the connective tissue massage alone, is one of the major factors which contributes to the formation of myogelosis in the area of chronic re-activation of trigger point.
In any scenario the fascia shortens first or it gets affected secondarily the complete elimination of the tension developed in the soft tissue depends on the combined efforts of working on the fascia and skeletal muscle it covers. This is the only way to achieve stable clinical results.
However we should go even further into the territory the article didn’t even mention despite that it is dedicated to the connective tissue. Besides forming envelopes for the muscles the superficial and deep fascia have another other equally important function. They provide stability between the different layers of the soft tissue.
Let’s look at Fig. 1 which shows the soft tissue arrangement in the area of the scapula and posterior shoulder. #1 indicates the superficial fascia which covers the posterior portion of the deltoid muscle which is indicated by #2; #3 indicates the location of fibrotic bridges which connect the superficial fascia to the subcutaneous tissue. The same fibrotic bridges connect deep fascia indicated by #4 which covers the infraspinatus muscle indicated by #5 and separate it from the posterior portion of the deltoid muscle (#2).
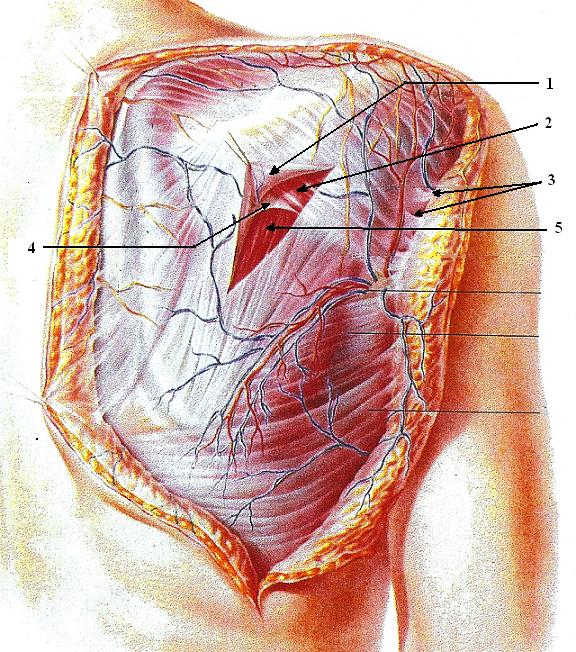
Fig. 2 presents the layer-by-layer cross section arrangement of the soft tissue in the same area, i.e. scapula and posterior shoulder.
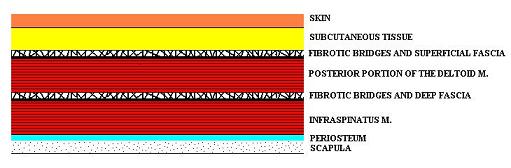
Fibrotic bridges seen on Fig. 1 (#3) and Fig 2 are one of the main elements responsible for the building up tension in the superficial or deep fascia. As soon as the bridges loose their elasticity, tension and scarification develop in the collagen fibers of the fascia.
The connective tissue massage protocol should address the superficial fascia and fibrotic bridges, which connect it to the subcutaneous tissue and skin and the article correctly describes ways to do it. However, the practitioner must examine and address the deep fascia as well. The only way to do it is to stretch the fibrotic bridges which control its tension by using massage strokes (especially kneading) on the superficially located muscles. In such case the lifting, stretching and mobilizing superficially located muscle (posterior portion of the deltoid muscle in our case) allows us to stretch the fibrotic bridges of the deep fascia and restore their normal elasticity. Thus article’s claim that practitioner who found tension in the fascia must address only the fascia itself misleads the readers, restricts their technical potential and contributes to the further fragmentation of the profession.
The final thought is sadness due to the fact that the author’s “…hands do not readily remember how to massage muscles” and that this information is a part of the seminars mentioned at the end of the article.
Let There Be Mud! Massage 162, Nov:26-30, 2009, by Phyllis Hanlon
A great article on mud treatment. It gives basic information about its application and products. The mud therapy is mostly used in spas, but at the same time it is a very powerful treatment tool in cases of osteoarthritis, tendinitis, etc.
Moor mud is the best quality for these purposes available in the USA. However for the optimal clinical benefits just application of the mud on the affected joint is not enough. The practitioner needs to use an active carrier which helps the active ingredients of the mud to penetrate into the local circulation.
The most effective carrier is electric current and the application of the TENS unit or any electric device with electrodes placed on the skin next to the mud will work great. In many cases the application of electricity is beyond the scope of the practitioner’s practice. In such case he or she may use a flow of photons for the same purpose. The simplest source of photons is a lamp with a clear bulb placed just over (approximately 12-15 inches) the part of the body covered with mud.
Category: Good Apples, Bad Apples