
The purpose of this section of the Journal of Massage Science to inform the practitioners about valuable articles that frequently go unnoticed, as well as to point to those authors and publications who exhibit low educational standards. We do not play politics and we are not associated with any publishing company or professional association. We are a completely independent voice and we promise you direct unbiased reviews based strictly on the science.
If the author of the reviewed article does not agree with our opinion, we will be more than happy to publish his or her response and have a productive discussion over the article’s subject.
At the end of the year we will recognize and reward the author of the most important publication(s) and point to the authors of the most unscientific publication(s). We hope this will help to raise the bar of published materials in massage journals for the benefit of the entire profession.
MASSAGE THERAPY JOURNAL

Evidence Informed Practice, Part II: Evaluating and Documenting the Results of Your Work. MTJ, Spring, V. 49(1): pp. 99-101, 2010, by M.B. Menard, PhD, CMT
The subject of this great article is a very important professional issue. The author advocated and explained the importance of proper documentation for the massage practitioners. The article also offered basic tools to document the initial examination and to evaluate treatment progress.
We bet that a very small number of practitioners do that regularly, and those who keep such documentation mostly work in a medical office or with insurance companies. In other words the practitioners are forced (in many cases) to document their treatment. We believe that a very small number of the practitioners realize the importance of proper documentation and fully understand its clinical value.
Documentation of the therapy is less important if the massage therapist is in the field of preventive massage therapy, e.g., practice of stress-reduction massage. However for those practitioners who build their career in the field of medical aspects of massage therapy the proper documentation becomes a great clinical tool. It gives the practitioner the upper hand in battling with any pathological condition in the human body.
Very frequently we hear from the practitioners that they don’t keep any records because they remember clients and their conditions. We guarantee that the practitioner will be shocked at how much important clinical information he or she forgets if this information was not properly recorded.
Let us say that you had a client with lower back pain and you successfully solved this case six months ago. Now you see the same client with the pain between shoulder blades in the middle back. What you found during initial evaluation and what you did during treatment will greatly help you to quickly solve his middle back pain.
Another advantage of proper documentation is your ability to form a database of the cases. Such database can be a great tool in promoting your treatments among physicians, chiropractors or physical therapists. With proper documentation you have actual proof of your successes and it will allow you to find out what abnormalities you encountered most frequently and what your personal rate of success is.
Finally, keeping records will help you to optimize your treatment protocols because you will be able to evaluate what techniques and protocols are more efficient, what you should additionally mastermind and what treatments are less effective and even useless. Keeping documentation of conducted therapies and their periodic analysis will enhance your professional performance. A positive by – product of keeping the proper documentation is the elimination from the arsenal of massage practitioners those techniques and modalities are useless nonsense because of their low clinical effectiveness.
Body Mechanics. Seven Keys to Healthy Neck Posture. MTJ, Spring, V. 49(1): pp.93-97, 2010, by J. Muscolino, DC
A great article! It addresses the important issue of how the client with chronic neck pain should behave in everyday life. Let’s consider that you start the treatment of the new client with cervical pain. The treatment doesn’t end in the therapy room because what the client does between sessions will greatly affect the duration and outcomes of the therapy.
In this article Dr. Muscolino provides seven very simple self-helping lifestyle adjustments the practitioner may recommend to their clients. Very good illustrations are a great help.
Easing the Constant Pain. MTJ, Spring, V. 49(1): pp.48-57, 2010, by Karta Purkh Singh Khalsa
An excellent article! It covers the topic of Fibromyalgia (FM) and does it in a very easy to read form with a review of recent scientific studies. It gives the reader the confidence to work on the client or it gives the client with FM a sense of hope in cases when no hope is left.
Another positive feature of the article are good illustrations of the tender point examination throughout the client’s body. The author cited Dr. P. Abaci: “Don’t just concentrate on the pain. You need a whole person approach” and we think it is a very true for the successful management of FM. The article greatly supports this basic statement.
Massage Today
Evaluating Neurological Symptoms. Massage Today, V10(3), 2010, by W. Lowe, LMT
The article raises the subject of the great importance of neurological symptoms associated with soft tissue abnormalities and evaluation of these symptoms. From article to article published in massage journals authors treated various abnormalities relaying mostly on local treatments, and these articles rarely even mentioned the fact that the pathological symptoms in many cases are the result of irritation or compression of the spinal or peripheral nerves on the upper segments of the body. The article discusses this important subject in an easy to understand and follow manner. Informative illustrations are of great help.
The Silent Progression of Kidney Infections and Stone Formation. Part 2.Massage Today, V10(3), 2010, by D.G. Alexander, LMT, MA, PhD
A very good article on the correlation between kidney infection and stone formation. What is very helpful is a list of the questions the practitioner may ask to determine if clients have potential in formation of the kidney stones. This is a very helpful practical tip.
Uterine Fibroids. Massage Today, V10(3), 2010, by E. Stillerman, LMT
A very helpful and educational article of the nature and formation of uterine fibroids, its clinical symptoms and treatment options. The author has provided helpful information on newly developed treatment methods for the patients with uterine fibroids and it shows her dedication in writing informative pieces.
Rib Pain “Can’t Get No Respect” Massage Today, V10(3), 2010, by E. Dalton, PhD
Bravo! What a great article! The author has exhibited excellent clinical skills and educational talent in order to explain the origin of pain in the middle of the back. It is true that in many cases the practitioners are knocking on the wrong door when they start the treatment of the pain between the ‘shoulder blades’. We highly recommend reading this important article.
Trigger Points in the Fibularis Tertius Muscle. Massage Today, V10(3), 2010, by D. Kent, LMT, NCTMB
A very good article on the evaluation and trigger point therapy of the fibularis tertis muscle. A very helpful part of the article are several tests which help to isolate and examine this muscle.
Stretching the Limits of Your Massage. Massage Today, V10(4):12; 18, 2010, by T.A. Schmidt, DPT, MS, OCS, LMT, CEAS
A great and very important article! It covers the history, science and basic principles of application of Muscle Energy Techniques (MET) which is one of the greatest contribution of American scientists in the manual therapy and medical massage field. The author does a great job of explaining the nature of MET and differences in the clinical application as well as providing helpful clinical recommendations which the practitioner may immediately put to work.
In times when a very simplified versions of MET (e.g. Isolative Stretching) dominates the filed this article gives the readers a better sense of what the bigger picture of MET is all about.
Multifidus: The Multi-Tasker. Massage Today, V10(4):17, 2010, by J. DeLany, LMT
A very good article which touches a frequently overlooked issue of the role the multifidus muscle plays in lower back pain. Very good illustrations help the reader understand the article topic. At the end of the article the author briefly addressed the treatment options and she tried to describe the way the practitioner should approach this muscle.
The description is a correct but it will be great if the author had provided a picture to actually show the practitioners the palpation and treatment of multifidus muscle. Work on multifidus muscle it is not an easy task if the readers have never learned it from any other source. It is difficult to learn it from description alone. This is the only minor disadvantage of overall a very good article.
Baby Massage Techniques. Massage Today, V10(4):1-3, 2010, by L.B.Rush, LMT
A very informative article on the basic requirements for baby massage for the healthy child. The article showed that the author has the knowledge and passion for her work with small important details emphasized.

Pain Caused by Low Back Ligaments. Massage Today, V10(4):10, 2010, by B. Benjamin, PhD
We have already discussed this issue advocated by the same author in his article published in December of 2008. Unfortunately, the author still stands behind the incorrectly presented information.
In this article he answers the following question:
An injured sacrotuberous ligament can cause pain down the back of the leg. True or false?
He answers this question as: True. This is its referred pain pattern.
The correct answer should be: False. The injury of sacrotuberous ligament itself will never send pain to the back of the leg. Now let’s get into the details one more time.
1. First of all the referred pain is the incorrect way to describe pain on the back of the leg which has originated from the lower back or gluteal area. The referred pain stays within the borders of the same anatomical segment. We would like to send readers to Travel and Simmons Trigger Point Manual where referred pain patterns from each muscle are presented on very informative diagrams. As you may see in illustrations in this publication the referred pain from the active trigger point in every muscle practically always stays within the same anatomical segment.
On the contrary, the pain which travels along three anatomical segments (gluteal area, thigh and leg) is called radiating pain. The pain pattern discussed in the article is associated with the irritation or compression of the spinal nerve or sciatic nerve and, to be more precise, with the tibial nerve portion of the sciatic nerve.
Specifically, for this review we scanned all major medical articles (earliest published in 1952) which experimentally and clinically examined the pathology of the sacrotuberous ligament. To our readers and the author we didn’t find any information which backed up the author’s claims that the injury of the sacrotuberous ligament is responsible for the pain radiation to the leg.
2. The sacrotuberous ligament is not easy injured. It is especially impossible to injury this ligament alone without traumatizing other more vulnerable anatomical strictures. This ligament can be injured as a result of direct trauma, but again, it will be the last to suffer or its injury can be a result of traumaof the hamstring muscles.
The author stated that injury of the sacrotuberous ligament “…is frequently confused (bold by JMS) with the hamstring injury…” This is not the correct way to describe the chain of events. The tension and spasm in the hamstring muscles as a result of injury and their consequent shortening are a direct cause of the tension in the sacrotuberous ligament (van Wingerden et al., Eur J Spine, Oct 2(3):140-144, 1993). For this reason the test described in the article (knee flexion against resistance) to differentiate between injury of the sactotuberous ligament and injury of hamstring muscles simply is not a valid examination tool for this case.
It seems that the author relied on old ideas of sacrotuberous ligament strained or injured because of tension developed in these ligaments as a result of the dynamic activity of the pelvis. Recent biomechanical studies showed that the previous concept of the sacrotuberous ligament as well as other pelvic ligaments playing a critical role in the dynamic movements of the pelvis is not valid anymore. As authors of the recently published study (Conza, Rixen, Plomp, J. Biomech., 2007 40(7):1500-1605) showed, the cutting of each separate ligament and exposing the pelvis to the vibration didn’t change the pelvis dynamic biomechanical model except by contributing to its stability. Earlier study (Vrahas, Hern et al, Orthopedics 1995, 18(3):271-274) made same conclusion.
Thus, the notion of the injury of the sacrotuberous ligament as a result of any cause except massive direct trauma of the pelvis is outdated. If one had such massive trauma of the pelvis the injury of sacrotuberous ligament is not a priority for the treatment.
3. There is a reasonable question as to why and how the article links the sacrotuberous ligament with the radiating pain to the leg. We are sure that the article confuses two different subjects.
The referred pain from the sacrotuberous ligament will never travel below the knee. In the majority of cases it stops on the upper or middle third of the thigh. If the client feels pain in the leg and there is no local cause of it, the client has a radiating pain along the sciatic nerve.
Instead of continuously raising the issue of non-existing pain radiation down to the leg in cases of injury to sacrotuberous ligament the author should mention that sacrotuberous ligament plays critical role in the compression of the pudendal nerve (responsible for innervation of genital and anal areas) between this ligament and sacrospinos ligament. As it was correctly pointed by Dr. R. Robert “The pudendal nerve is the king of the perineum”. Unfortunately, this important fact wasn’t even mentioned.
4. Why it is so important to distinguish between pain originated from the sacrotuberous ligament or for example from the irritation or compression of the sciatic nerve by the piriformis muscle? It seems that it is a minor issue and we pay too much attention to this unimportant subject.
However, in the clinical situation the incorrect presentation of this subject and subsequent incorrect approach to the treatment greatly reduces the effectiveness of the therapy.
Let us consider that the practitioner examines the new client with radiating pain to the posterior leg and now thinks (learning from the article) that this pain is a result of tension in the sacrotuberous ligament. He or she will build up an entire treatment protocol based on this incorrect notion while the real problem let’s say is tension in the pirifomis muscle. In such a case the article sent the practitioner knocking on the wrong door and it greatly diminishes the practitioner’s clinical effectiveness.
Basics of Oncology Massage. Massage Today, V10(4):10, 2010, by D.J. Razo
This short article addressed the basic principles of oncology massage. It is helpful for those practitioners who consider extending their practice in this direction. The article gives a very basic set of tool and this is the exact goal of this short piece.
Massage
Is Massage Safe for Clients Who Have Alzheimer’s Disease? Massage166:46-49, 2010, by S. Puszko, PhD
A great, very well written and helpful article! Considering that “Every 70 seconds someone is diagnosed with Alzheimer’s” and it “…is the seventh leading cause of death in the US” the issue is a very important for the affected individuals, members of their families as well as for the entire society in general.
The author provided the result of several recent studies which examined the impact of massage therapy on Alzheimer’s patients and shared with the readers her own protocol of working with this difficult category of the clients.
Of course, the massage therapy is unable to cure this debilitating disease, but at the same time it is important additional tool which helps keep Alzheimer’s Disease in check.
There’s A New Stone in Town. Carved, Quarried Basalt Massage Stones.Massage 166:30-34, 2010, by P. Mayrhofer
Hot stone massage is one of the greatest developments in modern massage therapy. We always thought that it will be very nice and helpful to have shaped stones for Hot Stone Massage. Now this is a reality! These tools are definitely essential help for the practitioners and it will be greatly appreciated by all clients. The website cited in the article as a resource is: www.naturestonesinc.com
Massage & Bodywork
Auth Method. A Guide to Forearm Massage. Massage & Bodywork, March/April: 73-77, 2010, by S. Auth
The subject of this article is massage using forearms. The author informs readers about the method of forearm massage she developed, and, of course, conveniently named the Auth Method.
In the article the author mentioned that the forearm massage wasn’t part of the curriculum in her massage school and she later developed it to save practitioners’ hands. The usage of forearms for the massage is technique as old as massage itself. We would like to send, those who are interested, to early images of massage therapy from ancient Egyptian tombs where forearm massage is clearly visible. Thus it was a bad curriculum in the author’s school if she wasn’t taught it there.
In the practical part of the article the author shows very basic applications which are used by practitioners all around the world without knowing about the Auth Method. Nevertheless, it is great that the author raises the question of importance of studying and using forearm massage techniques even in the form of the Auth Method.
However, the really troubling part of the article is how the author recommended the use of forearm techniques. According to the author she uses and teaches others to use only forearm massage techniques during entire session.
Ask yourself a simple question: Would you pay for a massage session where the practitioner uses only forearm techniques? By doing so the author automatically eliminates all kneading techniques (one of the most valuable), friction at the place of attachment, passive stretching, percussion, etc. In such a case the entire professional arsenal becomes a narrow minded and boring repetition of several similar strokes. In other words, the article advocates robbing the client of real treatment for the sake of “…keeping work-related injuries to a minimum”.
The kneading or friction techniques which author advocates to eliminate from the practitioner’s arsenal are not the causes of the professional injuries, but the incorrect body mechanics during their execution is. Approach to massage therapy recommended in the article is dead end for massage development and its clinical application or, in other words, it is a sign of professional incapability.
Let us see how the author tries to justify the clinical value of the Auth Method without the application of other massage techniques. The article concentrated on three major factors where the Auth Method has advantages when compared to the centuries old modern school of massage.
“The forearms are a bodyworker’s most prized tool…” It is simply sad to read quote like this one. Yes, forearms are more durable than hands but they are not the most prized tools, our hands are the most prized tools. As a matter of fact the majority of modern philosophers and evolutionists consider that our ancestors hands especially the factor of thumb opposition was a major instrument which contributed to the development of our brain during evolution. We would like to repeat that hand injuries are a result of incorrect body mechanics rather than massage techniques themselves.
2. Sensitivity
“With practice, the forearms are just as sensitive and agile as the hands, fingers, or thumbs”. How can anyone involved in massage or manual therapy can say something like that?
Let’s address this nonsense. The sensitivity of the hand or any other part of the body relays on two major factors:
The brain is very similar to the computer. The more space on the hard drive is available the more efficient the execution of the programs.
If the author opened basic physiology textbook before publishing this article she will find that skin on the fingertips contains at least 60 sensory receptors (excluding pain receptors) per square centimeter while the skin on the dorsal surface of the fingers as well as forearm contains only 6 sensory receptors per square centimeter.
Now let’s examine the factor brain capacity. Fig. 1 shows the most commonly use somatosensory map of the brain. This picture presents a cross section of the brain which matches various parts of the body of so-called ‘homunculus’.
Homunculus helps to illustrate what space in the cortex sensory information from different parts of the body occupies. For example the face is larger than the leg and this means that sensory information from the face occupies more space in the brain than sensory information from the leg.
The readers may even find out that sensory information from the peripheral receptors around the lips occupies more space in the brain than information from the receptors in the forehead because on the diagram area of the mouth is larger.
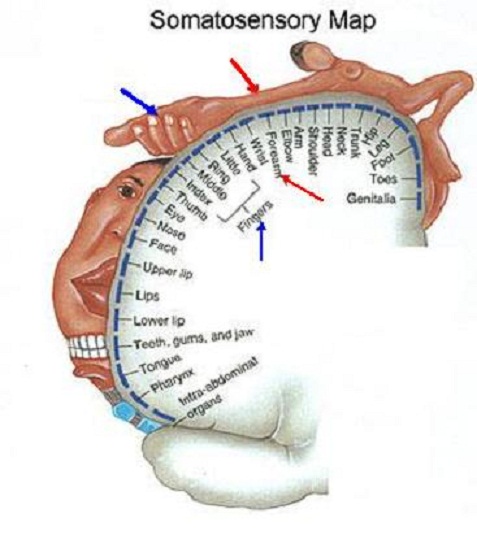
Fig. 1. Somatosensory map of the brain
From this very short trip to the basic of physiology the readers may see that the forearm has a much lesser number of sensory receptors, and there is much less room in the brain dedicated to process and analyze their input.
Thus the notion that the practitioner will be able to train his or her forearm to have sensitivity and ability of two points discrimination equal to the hand and fingers illustrates the author’s complete unfamiliarity with the subject. There is no way on this planet that the forearm may ever substitute for the hand. Those who think and spread this misinformation are simply dead wrong.
According to the article the forearms have more leverage when compared to the hands. The author illustrates this notion with the fact that “Your body will naturally drop to the first layer of tight tissue… as that layer of tissue releases, you will drop into the next layer of tight tissue”. However this is not a leverage advantage, because the correct body mechanics for every massage techniques requires the engaging weight of the body into each stroke and it is simply wrong to associate it only with the forearm or any other individual massage technique.
At the end of the article the author shares several Qigong Exercises to help practitioners to relieve body stress and tension. This is a good part of the article.
In conclusion: Please do learn (you may very well use Auth Method’ DVD or seminars) and use forearm techniques in your practice. Do not base your session entirely on one approach. Your sessions must be exciting, unpredictable and filled with creative energy. Never listen to those who wish to squeeze you into the box of artificial boundaries. This is a dead end of the profession.
Ten for Today. Hand Tools. Massage & Bodywork, March/April: 73-77, 2010, by R.Jones
A very good article which in the simple and helpful format educates the practitioners about correct usage of hands tools during massage therapy session. The entire article is arranged as a series of questions about hand tools and the author answers them efficiently. These questions cover many topics from the different hand tools to the ethical issues of their application.
Table Lessons. What Just Happened Here? Massage & Bodywork, March/April: 82, 2010, by D. Nelson
As always articles in this column are great. The author uses simple language when he describes his clinical cases. Articles like this one have great educational and inspirational value because they build up professional self-confidence in readers.
Functional Anatomy. Tibialis Posterior. Massage & Bodywork, 85-86, 2010, by C. Cael
Finally a correct article on palpation written by C. Cael! Everything is great: anatomy, physiology and palpation process. We hope that new upcoming pieces will be of the same quality!
Essential Skills. Adductor Muscle-Tendon Injuries. Massage & Bodywork, March/April: 90-95, 2010, by B. Benjamin
An excellent article on the injury and treatment options of the adductor muscles. There is one thing we would like to address, because it is very important for the practitioners who may deal with this abnormality.
Yes, if the patient has history of actual trauma this quote is completely correct. However there are many cases when the patient did not have history of the groin trauma but he or she exhibits clinical picture of injury of the adductors. In such cases the practitioner must examine upper quadratus lumborum muscle on the same side as well as femoral canal on the anterior inguinal area.
Patients with Femoral Nerve Neuralgia always exhibit local pathological abnormalities in the adductors. In many cases when the quadratus lumborum or iliopsoas muscles slightly irritate the origin of femoral nerve or nerve itself the patient produces clinical picture 100% identical to the injury of the adductors without complaining about any symptoms on the upper lower back or inguinal area.
If the practitioner encounters the patient with Femoral Nerve Neuralgia which mimics the injury of adductors and he or she approaches the treatment from the point of local injury the results of the therapy will be very disappointing. In such cases the local symptoms of tension in the adductors are consequences to the slight irritation of the femoral nerve and until nerve is freed by using proper treatment protocol these symptoms will come back.
Thus not all pain symptoms in the upper groin are associated with adductor injury and it is the practitioner job to determine this fact during initial examination. Otherwise he or she will waste efforts and patient’s money.
Fatty Liver Disease. The Nonalcoholic Spectrum. Massage & Bodywork, March/April: 97-101, 2010, by R. Werner
An excellent educational piece where the author presents the pathophysiology of the fatty liver disease, its origin, clinical symptoms and treatment options.
Myofascial Techniques. Working With Whiplash. Part 1. Massage & Bodywork, March/April: 108-115, 2010, by T. Luchau
An excellent article! Thank you for a smartly written and clinically important piece. We liked the analogy of the differences in clinical pictures of Hot and Cold Whiplash.
We would like only to add that besides causes of vertigo as a result of whiplash mentioned in the article, this complication can be triggered by tangling of hair cell receptors inside the inner ear because of the sudden impact and the same clinical picture of dizziness can be the outcome of compression of the minor occipital nerve in the area of the occipital ridge by posterior cervical muscles.
Category: Good Apples, Bad Apples