
In every issue of our Journal, you will find the Case of the Month, which we will select from the submitted ones. Everyone who uses MEDICAL MASSAGE PROTOCOLs in their practice may submit their cases for review, and we will share the best one with our readers in every new issue.
We didn’t receive an interesting submission to the Case of the Month for this issue of the Journal of Massage Science. However, we don’t want readers to miss the potentially important practical information from this section. This is why we decided to share with you an interesting case from our clinic.
Dr. Ross Turchaninov, Editor in Chief
MEDICAL MASSAGE vs ERECTILE DYSFUNCTION
The patient is a 42-year-old male. He works in finance. Recently divorced.
Initial Complains
Originally, the patient was treated at our clinic 3 years ago for Lower Back Pain and Sciatic Nerve Neuralgia as a result of tension in the piriformis muscle. His initial symptoms were on the left side and consisted of intense lower back and gluteal pain, which radiated to the left leg and the top of the left foot. His treatment was successful, and he attended sessions periodically for support.
Several months ago, he noticed a tingling on the left side of his penis’ head. Initially, he didn’t pay attention because he had numerous personal issues to deal with. In a month, he noticed the spread of tingling along the shaft while the head started to feel numb. He went to his family physician, who ordered several tests, and all of them were normal. His family doctor sent him to see a urologist. While waiting for the appointment with the urologist, he noticed a decrease in blood flow during the erection. The patient became greatly frustrated. The urologist didn’t find any pathological abnormalities and recommended him to see a neurologist, and prescribed Viagra. The medication restored the blood flow, but there were no changes in the decreased sensitivity.
Further examination and almost a month of tests by a neurologist didn’t reveal any abnormalities. Considering the emotional stress of divorce, the neurologist concluded that the patient suffers from a so-called conversion disorder. In such cases, the emotional or psychological problems the patient experienced convert into various somatic or visceral abnormalities. His advice was to continue to take Viagra, start to see a psychologist, and the condition would normalize by itself after his family issues had been resolved.
Initially, the patient became optimistic, but soon the clinical picture dramatically worsened. The medication wasn’t able to maintain the blood flow, and tingling and numbness spread to the scrotum. At this point, he decided to visit our clinic because he had become greatly frustrated and was desperate for help.
Clinical Examination
The patient seemed depressed, anxious, and exhausted. He almost cried when he said that he considers himself impotent. He also said that he became obsessed with his situation to the degree that he started to have problems with sleep.
The patient didn’t complain about any significant lower back pain. He felt the tightness in the hamstring muscles. He also noticed an uncomfortable sensation of heaviness in the area between the anus and the root of the penis. He felt a constant need to change position while sitting in a chair; otherwise, these sensations became very uncomfortable.
During examination of the lower back, he exhibited a positive Withdrawal Sign when moderate pressure was applied in the area of the left sacro-iliac joint. There was a lesser intensity of pain at the insertion of the tendons of the lumbar erectors into the sacrum.
The overall muscle tone of the hamstring muscles on the left side was significantly higher when compared to the right side. However, no trigger points were detected.
Considering his history of lower back pain and sciatica, we decided to approach his condition using a combination of MEDICAL MASSAGE PROTOCOLs for the Lumbalgia (i.e., lower back pain) as a result of tension in the lumbar erectors and Sacroiliitis.
We also recommended that the patient actively stimulate the skin in all areas with decreased sensitivity. The patient started to use intense friction, pinching, compression, electric vibration, and alternate application of ice and heat to all affected areas on the penis and scrotum.
MEDICAL MASSAGE PROTOCOL
1st week (1-3 sessions)
We used this combined protocol for three sessions with one-day breaks before the patient noticed increased blood flow and the appearance of what he described as ‘spontaneous erections’ during the day without any erotic stimuli. This was a very promising outcome, and the patient became very excited about the potential improvement of his health.
2nd week (4-6 sessions)
The blood flow continued to improve, and he was able to achieve an erection without taking Viagra or Cialis. However, he felt he needed to take medication because he still had problems with maintaining an erection during intercourse.
The patient mentioned that the sensation of heaviness in the pelvis is not getting better. Considering that this sensation was more likely a result of tension in the pelvic floor diaphragm, we instructed the patient to perform modified Kegel exercises twice daily.
3rd week (7-9 sessions)
The blood flow was completely restored, and the patient no longer felt numbness in the scrotum. However, the numbness along the shaft of the penis and especially the head didn’t change at all. The patient was able to maintain an erection without medication, but he felt that he didn’t have satisfaction because half of his penis remained numb. Also, the sensation of heaviness disappeared after self-application of modified Kiegel’s exercise.
4th week (10-13 sessions)
Despite all of our efforts, the sensitivity along the penis didn’t improve a bit. Considering the lack of progress in this area at the beginning of the 10th session, we decided to re-examine current clinical symptoms and adjust the treatment protocol.
Re-examination showed that the patient didn’t have the original clinical symptoms in all areas of the lower back and scrotum. However, the detailed examination of the left gluteal area revealed unusual clinical symptoms. The application of direct pressure along the sacrotuberous ligament and especially in the area of the pudendal canal immediately increased the intensity of the symptoms along the shaft and head of the penis. Now, the increased tone of the hamstring muscles has become an understandable factor and plays a significant role in the treatment.
To understand the importance of this information, I would like to briefly discuss the subject of the pudendal nerve and pudendal canal. Figure 1 illustrates the pathway of the right pudendal nerve and the location of the pudendal canal. Notice that the pelvis is split in half along the vertical axis; therefore, you are looking at the medial side of the right pelvis.
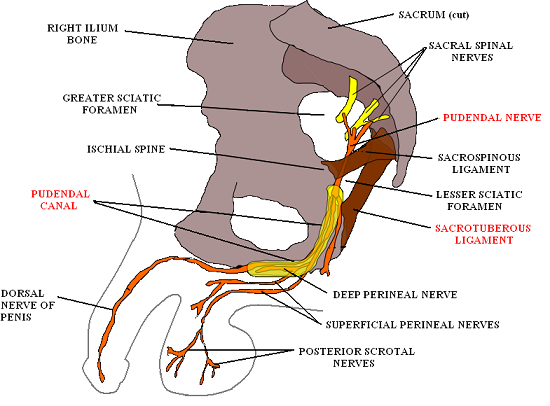
Fig. 1. Pudendal nerve and pudendal canal
(Häggström, Mikael (2014). “Medical gallery of Mikael Häggström 2014“. Wiki Journal of Medicine (1) 2. DOI:10.15347/wjm/2014.008. ISSN 2002-4436. Public Domain)
The pudendal nerve, which is also called ‘king of the perineum’, originates from S2-S4 spinal segments. It splits from the S2-S4 spinal nerves just before they enter the sacral plexus (see Fig. 1). After that, the pudendal nerve exits the pelvis via the infrapiriformis recess medially to the sciatic nerve (see Fig. 2). Almost immediately, it enters the pelvis again through the lesser sciatic foramen. After this, the nerve gets into the pudendal canal (see Fig. 1 and Fig. 2) located along the medial surface of the obturator internus muscle. The pudendal nerve provides sensory and motor innervation to sex organs as well as the urinary bladder and anal sphincters.

Fig. 2. Right pudendal nerve on the posterior gluteal area
The pudendal canal is formed by the obturator internus fascia and also contains internal pudendal arteries and veins. The most problematic part of the pudendal canal is its entrance, where sacrospinous and especially sacrotuberous ligaments (see Fig. 1 and Fig. 2) may contribute to irritation or compression of the pudendal nerve in the pudendal canal. The chronic tension in the hamstring muscles is responsible for the tension in the sacrotuberous ligament, which in turn may irritate the pudendal nerve in the pudendal canal and produce Pudendal Nerve Neuralgia. This is the only nerve entrapment that the sacrotuberous ligament is responsible for.
As soon as irritation of the pudendal nerve was detected, the treatment of our patient was redirected to this area. The MEDICAL MASSAGE PROTOCOL to decompress the pudendal nerve includes three steps:
1. Work on the hamstring muscles to restore their normal muscle tone.
It helps to decrease tension in the sacrotuberous ligament and assists in decompressing the pudendal nerve. We used a combination of kneading in the inhibitory regime, longitudinal and cross-fiber friction, passive stretching, and postisometric muscle relaxation.
2. Work in the gluteal area
The goal is to decrease tension in the gluteus maximus muscle and especially the piriformis muscle. We partially used the protocol for the Piriformis Muscle Syndrome.
3. Work on the sacrotuberous ligament and at the entrance to the pudendal canal
The final part of the session targeted the sacrotuberous ligament. The intensity of all applied techniques was correlated with the patient to prevent any possible traumatization of the pudendal nerve during treatment. Friction along and across the sacrotuberous ligament, permanent, fixed electric vibration, local stretching of the ligament, as well as general passive stretching of the left lower extremity, were used.
The video below shows the application of the friction along the sacrotuberous ligament. The purpose of this video is to guide practitioners to the area of pudendal nerve decompression.
Decompression of the pudendal nerve was the final piece of the puzzle, which allowed us to completely restore sensitivity along the left side of the penis. The patient currently visits our clinic once a month for supportive therapy. He also uses an inversion table and regularly stretches his lower back, and he hasn’t experienced any episodes of decreased blood flow or sensitivity.
We observed positive results for three months. After several months of stress and misery, the patient completely recovered, and it took only 13 sessions of medical massage therapy to obtain stable clinical results and give the patient his life back.
How did all of this happen? Here is the most likely scenario of abnormality.
The patient had chronic lower back problems, which eventually caused tension in the hamstring muscles on the left. This tension affected the sacrotuberous ligament, which irritated the pudendal nerve at the entrance in the pudendal canal, with the following pathological changes in the sensory and motor innervation of the perineum.
What treatment options does modern American medicine offer a patient with Pudendal Nerve Neuralgia? To answer this hypothetical question, we will consult a recent comprehensive medical source on this subject: Antolak. Genitourinary Pain & Inflammation. Diagnosis & Management (2008). The only two options described are:
1. Pudendal Nerve Perineal Injections
A set of three monthly cortisol injections is recommended. Two under the sacrotuberous ligament, with the last one into the pudendal canal itself. This treatment is successful in 70% of cases during the first six months (Bensingnor et al., 1996). Afterwards, some patients start to exhibit similar symptoms, and the treatment is usually repeated.
Another problem concerns the last (third) injection, due to the frequent complications associated with this procedure, which may cause additional damage to the pudendal nerve. Because the injection needs to be done into the pudendal canal and the nerve tightly fits the canal, even modern diagnostic equipment doesn’t protect the physician from injecting medication into the nerve itself or the perineurium. This significantly increases the recovery time. This is why cortisol injections for Pudendal Neuralgia are practiced in a relatively small number of clinics.
2. Surgical Decompression of Pudendal Nerve
Surgical decompression of the pudendal nerve is also a questionable procedure. ‘Thirty to forty percent of patients fail to have significant relief following the surgical intervention’ (Antolak, 2008).
Another quote (from www.chronicprostatitis.com) states:
“Many people who have decompression of the pudendal nerve surgery are still in great pain years later. Only a small handful of doctors will do this operation. It is not mainstream medicine. The operation costs US$25K-$40K and most insurances will not cover it”.
A couple of final thoughts. As you may see, manual decompression of the soft tissues in the gluteal area using Medical Massage to free the pudendal nerve from irritation is not even mentioned in the medical sources. Since the accepted treatments are questionable from the perspective of their results and frequent side effects, the patients are left in limbo, and it ruins their lives. At the same time, therapists often don’t realize that their fingers are supposed to be the first line of defense in this and many other clinical cases.
Medical Massage saved our patient a great deal of money and precious time in his personal life. Thus, manual decompression of the pudendal nerve is a crucial and initial step in the treatment of Pudendal Neuralgia. Only after it fails should other, more invasive treatment options be considered.
Don’t waste time and join the Science of Massage Institute’s Medical Massage Certification Program. Our training, based on medical science and clinical expertise, has forever changed the massage practice of our former and current students. Visit SOMI’s main educational website for details: www.scienceofmassage.com
Antolak S.J. Pudendal Neuralgia. Genitourinary Pain & Inflammation. Diagnosis&Management. Edited by J.M. Potts, MD, 2008
Bensingnor M.F., Labat J.J. Robert R., Ducrot P. Diagnostic and Therapeutic Nerve Blocks for Patients With Perineal Non-Malignant Pain. 8th World Congress on Pain, 56, 1996.
ABOUT THE AUTHOR

Dr. Ross Turchaninov
Please click here for the author’s Bio: https://www.scienceofmassage.com/editorial-board/
Category: Case Studies
