
In the July-August, September-October, and November-December 2010 issues of JMS we published a three part article on TMJ dysfunction and in Issue #1of 2011 we published a follow up on the same subject. We tried to present to the readers comprehensive information as much as possible on the subject of TMJ pathology as well as available massage and manual therapy treatment options.
We did not discuss the critically important issue of intra-oral treatment of the TMJ dysfunction in either article. Unfortunately, from the legal point of view, the manual treatment in body cavities is outside the scope of the massage profession, even if the practitioners have proper training. In some states, it is even prohibited to be performed by chiropractors and physical therapists. This was the reason we didn’t include the protocol of intra-oral treatment for TMJ dysfunction.
Mrs. Gail Falzon, RN noticed the absence of this important information and contacted us offering an excellent answer to this problem. The MyoFree® Self-Massage Tool which she developed allows the patient to conduct self-treatment either learning on their own or under the practitioner’s guidance and supervision. In such cases the practitioner works on the outside addressing the externally located masticatory and cervical muscles, while the patient at home is able to address the inner masticatory muscles while supporting the work of the practitioner on the external ones.
We are sure that her elegant solution is a very important tool for everyone who works on patients with TMJ dysfunction, headaches and atypical face pain. First of all, it allows those involved to avoid legal controversy. Secondly, it involves the patient into the treatment process, which is a great psychological tool. Thirdly, it allows individuals to avoid technical difficulties that practitioners frequently face when they use intra-oral treatment. These difficulties are the result of the inability of the patient to open their mouth wide enough so that the practitioner is able to conduct effective therapy or when the practitioner has large hands and fingers while the patient’s mouth is anatomically smaller.
Thus we see the MyoFree® Self-Massage Tool and instructional video as a very important treatment system. This is why we would like our readers to consider the article below as an important professional piece rather than typical advertising.
CRANIOFACIAL PAIN SYNDROMES AND INTRA-ORAL TRIGGER POINTS
According to medical statistics, muscle dysfunction accounts for 85% of all pain syndromes. This is especially true for those suffering from craniofacial pain, including TMJD, headaches, atypical face pain (sometimes diagnosed as neuralgias) and cervical pain. Patients presenting with head, neck and jaw pain are sometimes challenging as there can be multiple components to assess and treat.
According to the National Institute of Dental and Craniofacial Research, the most common form of TMJD is myofascial pain, yet it is not taught in dental schools. In addition to bite splints, dental professionals use modalities such as biofeedback, external TENS and medications to relax the muscles.
Attempts to relax the muscle simply cause an active trigger point (TP) to become latent leaving the impression that all is well. It has been an enormous challenge to educate the dental community on the difference between “relaxing” muscle and “releasing” muscle dysfunction.
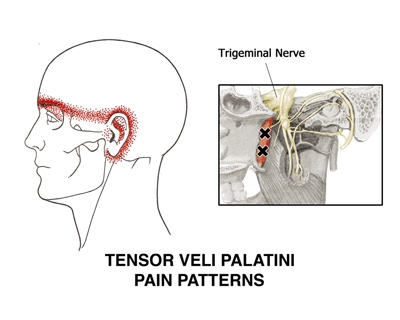
Because latent TPs (not causing an active pain complaint) can still decrease the range of motion, weaken the muscle and pull on bony attachments, it is important that we, as clinicians, not only correct the myofascial component, but also teach the patient how to self-treat when TPs become active again causing a myriad of painful symptoms and referred pain. (See Figure 1).
There have been many scientific and clinical publications pointing to TP infestation as either the central cause or significant contributor to painful syndromes and myofascial disorders such as seen in TMJD and other craniofacial pain (Simons et. al., ; Fricton, 1985; Fricton, 1999; Mackley, 1999, Alverez et al., 2002).
In a study involving 300 patients who all had been involved in a motor vehicle accident, the most common clinical findings indentified on medical evaluation were the following; jaw pain, neck pain, post-traumatic headache, jaw fatigue, and severe TMJ crepitus or clicking. The most common diagnoses in order were: masseter muscle trigger points, closing jaw muscle hyperactivity, and advanced disc derangement. (Friedman, et al., 2000).
Intra-oral TPs are often the underlying cause of headache and face pain but our society is more versed in prescribing medications which cover up the actual “source” of pain. Nothing is quite as gratifying as watching a patient diagnosed with Trigeminal Nerve Neuralgia discover that his or her pain is actually from a TP rather than true nerve damage. I’ve witnessed several patients get off multiple anti-seizure medications prescribed for nerve pain they didn’t require in the first place. It is my personal goal that intra-oral trigger points would be ruled out before giving a patient a hopeless diagnosis of trigeminal neuralgia or tic doulourex.
INTRA-ORAL TRIGGER POINT RELEASE
Intra-oral TP work is slowly becoming more common in therapy practice but is not the norm for therapy curriculum in our massage and PT schools. There are five major muscle groups found inside the mouth, which also include other surrounding muscles. For example the tensor veli palatini and internal pterygoids located in the roof of the mouth can be the cause of tension type headache, pain behind the eyes and sinus pressure. Dr. David G. Simons, MD agreed with the referred pain patterns shown in Fig. 1 although this particular one is not found in the current TPM.
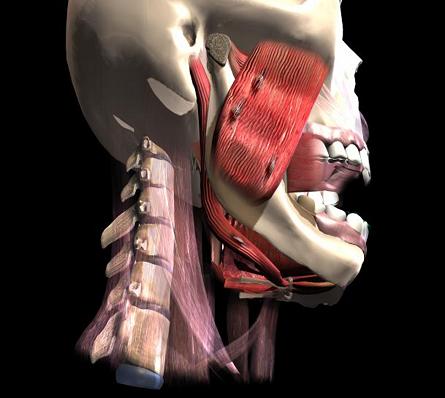
TPs are palpable contraction knots (see Fig. 2) or taut bands within the muscle/fascia that will ultimately change or alter muscle tension which can lead to secondary problems of internal derangement, arthritis, and/or faulty joint mechanics leading to ultimate joint erosion and breakdown.(Peroz, et al., 2002) Whether primary or secondary, the presence of TPs can perpetuate disability and worsen the prognosis if they are not considered and treated. An intricate pathway of nerves and blood vessels run through the muscles of mastication. Any disruption of normal function can lead to severe pain.
Personally, after suffering a whiplash and closed head injury in a MVA, it not only exacerbated a pre-existing TMJ disorder, but also caused me to have headaches around the clock. There seemed to be no medication or solution to help ease the pain and I was convinced by an oral surgeon that I needed a complete reconstructive jaw surgery. Not only did the surgery not work, it made the pain worse as I endured yet another two years of braces to correct the bite.
Desperate for help, I asked for a physical therapy referral and was incredibly fortunate to find a PT well versed in treating TMJD and headaches. She taught me how to self-treat using intra-oral TP release techniques, and for the first time, I experienced true pain relief that surprisingly was almost immediate. Because the treatment was so profound, I began teaching and treating others while continuing research efforts. It soon became evident that both reaching these muscle groups and following the release response all the way through was near impossible with the fingers and thumbs alone.
The MyoFree® SOLUTION
Based on years of research and product development, the patented MyoFree® Solution was born. The self-help “kit” consists of the easy-to-use MyoFree® Self-massage Tool (see Fig. 3) and the easy-to-learn, Inside-Outside™ technique. The instructional DVD uses 3D animation of the muscle groups to teach the location and treatment of intra-oral TPs using ischemic pressure. A full-color Quick Start Guide is also included showing an open mouth diagram and written instructions to compliment the video. A carrying case is included for travel and safe storage. (Note* The MyoFree® Massage Tool is for Patient Use Only!)

Inactivating the TPs from both sides, if possible, renders much more effective results. Also, a problem with most patients is the inability to treat the tensor veli palatini and internal pterygoids found in the roof of the mouth without eliciting a gag reflex. The MyoFree® massage tool (see Fig. 3) is small in diameter which allows even those with severe hypomobility of the TMJ to self-treat. One end of the device is shaped like a golf-tee and mimics the thumb. The other end is a very small ball and was designed to treat the attachment area of the lateral pterygoid which is located in a very small anatomical notch. Practitioners often complain that they can’t even reach this area with their pinky finger as it is so small and hard to reach.
There are two videos I would like to share with readers as examples of clinical application of the MyoFree® Self-Massage Tool. The first video presents the intra-oral treatment of tension and active trigger points developed in the medial pterygoid muscle. As readers know, this muscle is accessible for the direct therapy only using an intra-oral approach. The MyoFree® Self-Massage Tool eliminates necessity of intra-oral treatment conducted by the practitioner to achieve stable clinical results while involving the patient into the treatment process.
The MyoFree® Self-Massage Tool has another important benefit; its regular application by the patient between treatment sessions when the practitioner concentrates on the external treatment and re-alignment of the TMJ is very effective.
The second video demonstrates self-application of the MyoFree® Self-Massage Tool on the masseter muscle, which is usually targeted by the practitioners during external therapy. The MyoFree® Self-Massage Tool allows the patient to work on the masseter muscle combining external and intra-oral approaches at the same time.
An important advantage of the MyoFree® Self-Massage Tool is its future re-application by the client to maintain pain and tension free TMJ/headache symptoms after the entire treatment course is over.
Most therapists consider Dr. David G. Simons, MD to be the “father” of TP therapy since he co-wrote the Trigger Point Manual with Dr. Janet Travell. After watching the DVD and using the MyoFree® massage tool on himself, Dr. Simons wrote a two page testimonial to the dental profession on the importance of intra-oral TP release and why the MyoFree® device is so effective. His testimonial and other resource materials can be found at www.tmjpainsolutions.com
SUMMARY
Anyone who has suffered a head injury, whiplash, has TMJD and/or headaches should be made aware of these self-help techniques as part of a comprehensive approach to the rehabilitation. We, as therapists, pride ourselves on comprehensive home programs and providing knowledge that empowers a patient to become involved in their own wellness. The presence of TPs can be primary or secondary, but either way, can perpetuate disability and worsen the prognosis and interfere with primary interventions if not considered and treated. Left untreated, TMJD can become progressively worse and cause permanent damage within the tissues.
Trigger points have a sensory component but can also manifest as tension altering entities which, over time, can lead to uneven bite mechanics and restrict mouth opening. (Djkstra, et al., 1999). Research shows that TPs are a common component of diagnoses related to the head, neck and jaw. Intra-oral TP release has a huge impact on not only the muscles of the face and jaw, but also has a remarkable cervical component. Any therapy that can eradicate or control TPs should eventually become a standard part of the total treatment intervention for these difficult to treat conditions.
The MyoFree® Solution is a life-long, self-help, pain-relief system that teaches a patient how to self-manage their muscle pain symptoms for the rest of their life! The real beauty of the system is that anyone can easily learn the techniques. If you would like to learn these techniques, you will add a new important modality to your current practice and help desperate patients.
OTHER IMPORTANT FACTORS TO CONSIDER
There is never a single modality of treatment for these complicated diagnoses, but because intra-oral trigger point release is such a critical part of the pain puzzle, pairing it with existing treatments render far more beneficial results. Also important, of course, is teaching stretch and strengthening exercises, evaluating posture from the feet up, body mechanics, pelvic tilt and other perpetuating factors that can lead to the formation of TPs. Chemical imbalances and nutritional factors (Ferritin, Vitamin B1, Vitamin B6, Vitamin B12, Vitamin D, Serum Folate, Calcium, TSH, and serum magnesium and potassium) should also be considered in the overall evaluation of muscle pain and dysfunction.
The MyoFree® Solution is available at www.pressurepositive.com and retails for $59.00. Wholesale and health professional inquires are welcome. +1-800-603-5107.
Fricton JR. Masticatory myofascial pain: an explanatory model integrating clinical, epidemiological and basic science research. Bull Group Int Rech Sci Stomatol Odontol., 1999. Jan-Feb; 41 (1): 14-25.
Alverez DJ, Rockwell PG. Trigger Points: diagnosis and management. Am Fam Physician, 2002. Feb 15; 65(4):653-660.
Mackley RJ. Role of trigger points in the management of head, neck and face pain. Funct Orthod., 1990. Sept-Oct; 7(5):4-14.
Fricton JR, Kroening R, Haley et al. Myofascial pain syndrome of the head and neck: a review of clinical characteristics of 164 patients. Oral Surg Oral Med Oral Pathol., 1985. Dec; 60(6):615-623.
Peroz I, Tai S. Masticatory performance in patients with anterior disc displacement without reduction in comparison with symptom free volunteers. Eur J Oral Sci., 2002. Oct; 110(5):341-344.
Friedman MH, Weisberg J. The craniocervical connection: a retrospective analysis of 300 whiplash patients with cervical and temporomandibular disorders.Cranio, 2000. Jul; 18(3):163-167.
Djkstra PU, Hof AL, Stegenga B et al. Influence of mandibular length on mouth opening. J Oral Rehab., 1999; 26:117-122.
Gail Falzon, RN is a myofascial practitioner who specializes in craniofacial pain disorders. She treats patients in southeast Michigan, teaches other professionals and speaks at national conferences for therapists and other medical/dental clinicians who work with TMJD, headaches and atypical face pain. She is the founder of TMJ Pain Solutions and the Inventor of the MyoFree® Solution. More information can be found at www.tmjpainsolutions.com andwww.facebook.com/tmjpainsolutions.
Her contact information:
TMJ Pain Solutions
7446 Lochmoor Dr.
Ypsilanti, MI 48197
+1-734-277-5711
gail@tmjpainsolutions.com
Category: Medical Massage