
By Dr. Ross Turchaninov
We continue our series of articles under the general name, “How Massage Therapy Heals The Body” (please refer to issues of Jan/Feb, 2010; Mar/April, 2010; #3, 2011: #4 2011, JMS). In the previous issue of JMS (#3, 2014) we started a new topic: the modern science of pain from a massage therapy point of view. In Part I of this article, we discussed the cornerstone of modern understanding of pain – The Gate Control Theory of Pain (GCT) developed by Professors R. Melzack and P. Wall in 1965.
In 1990 Professor Melzack made a new step in the science of pain by introducing the Neuromatrix Theory of Pain (NT). This theory was finalized in cooperation with another world-renowned scientist, Professor J. Katz. The NT is the subject of this article, and we would like to emphasize that this article must be read only after Part I, which was published in #3 issue of JMS.
Recently, NT has created a wave of misunderstandings and misrepresentations in the community of somatic practitioners among chiropractors, physical therapists, and massage practitioners. There is a significant chance that as some people read this article, they will have already signed up or are waiting to participate in a seminar or webinar on the subject of pain and massage therapy. Our research indicates that in many cases, these continuing education classes are based on a misunderstanding and misrepresentation of NT, whether intentional or not. The situation had become so dire that we felt compelled to contact Prof. Melzack and Prof. Katz for clarification on these important subjects for the somatic practitioner community. We published their interview and our review of the current situation with GCT and NT in #4 issue of JMS.
Before addressing unscientific claims built around NT, we need to carefully go over the basic concept of NT. We will use the most frequently cited article on this subject as a source (Mezlack and Katz, 2013).
Although both theories are equally important components of our understanding of modern pain science, NT is more complex than GCT, as it also incorporates philosophical concepts. We will attempt to explain it simply, but it still requires the reader’s attention and the ability to analyze scientific data. Please sit tight and follow the text and illustrations we provide. Here it goes:
THE ESSENCE OF NEUROMATRIX THEORY
After the formulation of GCT, Prof. Mezlack continued his scientific exploration of pain. Eventually, he concluded that GCT doesn’t answer all the questions that clinical reality presents to scientists. The first step in building NT was the publication of the article by Professors Melzack and Loeser in 1978. In this paper, the authors described cases of phantom pains developed in paraplegic patients after a trauma that caused complete section of the spinal cord.
Usually, phantom pain, as a clinical phenomenon, is associated with pain in the limb after it was surgically removed due to severe trauma or cancer. In these situations, the patient’s brain, spinal cord, and peripheral receptors are still functioning perfectly together. Only what is lost is part of the limb. The patient feels phantom pain in this missing limb, as if it is still functioning.
However, in cases of paraplegic patients, the severe spinal trauma completely severed the spinal cord, and the brain lost any chance of getting sensory input from the parts of the body below the spinal injury. Prof. Melzack and his co-author were perplexed by this phenomenon. How can the patient’s brain form pain sensation in the form of phantom pain below the level of injury when the brain has lost all communication with the tissues there? The only explanation was that the brain, on its own, is capable of generating pain without any sensory input from peripheral receptors. At that time, it was truly a revolutionary idea!
Further studies and experiments conducted by Prof. Melzack and his associates allowed the formulation of a new step in our understanding of pain in the form of NT. Fig. 1 illustrates the concept and basic components of NT. This diagram consists of three parts: input to the neuromatrix, the neuromatrix with the neurosignature, and the neuromatrix’s output to various areas of the brain, which produce different responses.
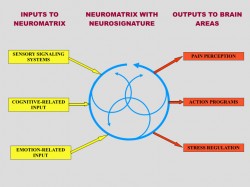
Fig. 1. Conceptual model of NT (Melzack, 2001)
1. INPUT TO NEUROMATRIX
As you can see in the left side of Fig. 1 (yellow squares) there are three major inputs into the neuromatrix:
a. Cutaneous, visceral and musculoskeletal input (i.e., sensory signaling system).
This part of the input is the next step in the normal function of the Gate-Control System. As we discussed in Issue #3 of JMS, T-cells (or Transmissions Cells) in the posterior horns of the spinal cord transfer the sensory information they received from the peripheral receptors, including nociceptors located in the soft tissues, all way to the neuromatrix located in brain (see Fig. 2 in GCT article in Issue #3, JMS).
This is a very important segment of NT since some massage “educators” deny the peripheral origin of pain and insist on its solely central origin. We will address this issue later.
b. Memories of past experience, attention, anxiety (i.e., cognitive-related input).
This type of input is an absolutely revolutionary concept. Let’s say that the paraplegic patient, during his years before spinal injury, fractured his leg. Of course, during this traumatic event, he experienced acute pain, which eventually subsided during fracture healing. After he sustained the spinal cord injury, and now the brain doesn’t have any sensory input from the extremity, which was once broken, the patient suddenly starts to feel phantom pain in the leg in the area of the fracture. In such a case, the memory of pain associated with the fracture was ‘imprinted’ into the neuromatrix, and now the brain itself ‘recreates’ this pain in the form of phantom pain, despite the fact that due to the spinal cord injury, there is no communication between the CNS and the once-injured leg.
Similar explanations can be projected to situations well known to somatic practitioners. An excellent example is Fibromyalgia, which is a somatic abnormality with a very strong psychological or central component. In Fibromyalgia patients, long-lasting chronic pain, which initially originated in the soft tissues, leaves its imprint in the neuromatrix. Now the brain starts to generate pain perception based on these previous pain experiences, in combination with anxiety and continuing pathological sensory stimulation from the affected soft tissues. Thus, the chronic pain starts to feed on itself, devastating the patient’s life.
c. Stress which affects the limbic system (emotion-related input)
Acute or chronic stress has a devastating effect on the body. According to a revolutionary concept by Prof. H. Selye called General Adaptation Syndrome (1955), modern medicine sees chronic mental, emotional, and physical stress as major factors in the development of various somatic and visceral disorders in our body.
The first negative outcome of stress is excessive activation of the sympathetic nervous system and release of cortisol into the bloodstream. It is a normal body’s protective response to any type of stress. However, the constant increase in cortisol levels associated with chronic stress has a devastating effect on the body. Cortisol elevates blood sugar, breaks proteins in the skeletal muscles and suppresses the immune system.
“Sustained cortisol release, therefore, can produce myopathy, weakness, fatigue, and decalcification of bone… it suppresses the immune system”.
(Melzack and Katz, 2013)
These effects contribute to the chronic pain and are especially important since part of the brain’s limbic system, called the hippocampus, is responsible for breaking down active cortisol. Changes in the limbic system due to negative emotions associated with pain and stress can exhaust the limbic system, decreasing its ability to break down cortisol and maintain a normal level in the bloodstream.
Conclusion: these three inputs to the neuromatrix equally contribute to the final formation of pain perception by the brain. In all cases of chronic pain, these inputs act at the same time by contributing to the formation of overall pain perception.
2. NEUROMATRIX AND NEUROSIGNATURE
The middle part of Fig. 1 (blue circles) illustrates the position and role of the neuromatrix in brain function, formation of pain, and other outputs. First let’s define what the neuromatrix is. According to Prof. Melzack and Prof. Katz (2013) the neuromatrix is a “widespread network of neurons that consists of loops between the thalamus and cortex as well as between the cortex and limbic system”
Thus, the neuromatrix is located in the upper echelons of the CNS. Its neurons unite three critical parts of the brain: the thalamus, which is a major relay station to determine what part of the cortex must be activated and by what stimuli; the limbic system, which controls our emotions; and the cortex, as a mainframe computer, which creates motor output to control body functions. These neural loops are shown as the circular arrows in the middle part of Fig.1.
So how does the neuromatrix work? As a result of various events we discussed above in the left side of Fig. 1, the neuronal loops of the neuromatrix are activated and they start parallel production of cycling nervous impulses. This cycling synthesis and processing of information allows the neuromatrix to produce in parallel several possible pattern of action as a response to the stimuli. The unsuitable ones are eliminated one by one until the most appropriate one for these particular circumstances emerges.
In a sense, the neuromatrix is a system that helps the brain to quickly eliminate wrong choices and find the best answer to the multiple-choice question that it encounters every second of our lives. All our experiences, like chronic pain, jealousy, envy, etc., have their imprint in the neuromatrix, and these existing imprints can be easily activated by new sensory triggers, past memories, or emotions.
Prof. Melzack and Prof. Katz called these areas of the neuromatrix associated with chronic pain, various emotions, past memories or analyzed sensory inputs – neuromodules. These neuromodules compose the combined output of the neuromatrix, which is synthesized there, and it is called a neurosignature.
Another critical role of the neuromatrix is the formation of our body self-awareness. Millions of various factors, from basic sensory stimulation of the skin to previous pain memories or long-ago negative emotions and stress, leave their imprint in the neuromatrix, which produces a range of sensations, from sensing temperature changes to chronic pain.
For example, a person who experiences chronic pain as a result of an injury also feels fluctuations in surrounding temperature, body position at that moment, the pressure of a chair, the smell of food, the ring of a cell phone, etc. Let’s say that the same individual who suffers from chronic pain while sitting at a table suddenly sees images of a car crash on TV. It reminds him of his own car accident and trauma, and at this moment, he feels that his pain is getting worse.
Prof. Melzack and Prof. Katz made the following analogy to describe the neuromatrix’s role in forming our body self-awareness.
“Like violins and brasses of a symphony orchestra, where each comprises a part of the whole; each makes its unique sound contribution yet is an integral part of a single symphony which varies continually from beginning to the end.”
Conclusion: Thus, all our experiences from hot/cold sensation to pain are synthesized by our brain in the form of a neurosignature, according to the initial triggers which are presented in the left part of Fig. 1. This neurosignature is continually projected to the corresponding parts of the brain creating body self-awareness which allows us analyze and fully interact with the very complex reality surrounding us.
3. OUTPUTS TO THE BRAIN
The right side of the Fig. 1 (red squares) illustrates various outputs of the neurosignature to the brain.
a. Pain perception
According to Prof. Melzack and Prof. Katz, pain perception synthesized by the brain includes sensory, affective and cognitive dimensions and thus is a very complex output.
b. Action programs
Action programs include voluntary actions like our movements and involuntary actions like gastric juice secretion when we are hungry.
c. Stress-regulation programs
Body’s response to acute or chronic stress is a very important output. It includes regulation of cortisol, noradrenalin, dopamine, endorphin production, and the immune system’s activity.
Conclusion: The final output to the brain is the result of complex interactions of initial triggers delivered to the neuromatrix by the Gate Control System or originating in the neuromatrix itself.
This very short review of the Neuromatrix Theory is based on publications by Prof. Melzack and Prof. Katz (2013). One more time we would like to emphasize that according to the authors of NT, it describes events in the brain itself after the Gate-Control mechanism has already been activated and finished its role in the formation of the pain perception.
PROFESSOR G.L. MOSELEY’S WORK
The Neuromatrix Theory of Pain in the beginning of 21st Century greatly impacted modern medicine the same way the Gate Control Theory of Pain did in the middle of 20th Century. NT gave birth to many great clinical ideas which improved our ability to understand and control the patient’s pain-analyzing system. One example is the work of Australian neurologist Professor G.L. Moseley, who deserves a lot of credit for his contribution to the science of pain.
Unfortunately, his work was misinterpreted by many somatic practitioners, including chiropractors, physical therapists, and massage therapists, and as a result, many unscientific ideas began to proliferate, especially within the massage therapy community. These ideas were immediately adopted by ‘educators’ who began to disseminate them through seminars and webinars, confusing practitioners and diminishing the clinical value of massage therapy. Before we discuss this subject, we need to discuss Prof. Moseley’s work and his contributions to pain science.
Prof. Moseley’s work is mostly based on the NT developed by Prof. Melzack. Prof. Moseley concentrated on the critical role the brain itself plays in the formation of pain perception. His studies confirmed that to successfully control the pain, analyzing system practitioners must take into account various neurological events within the brain.
He and his co-authors are entirely correct, as any chronic pain carries a significant so-called central component. In some categories of patients, e.g., phantom pains, Complex Regional Pain Syndrome, Fibromyalgia, etc., the central component of pain eventually starts to play the leading role in the pain that patients suffer from.
Besides studying and examining the role of the brain in pain perception, Prof. Moseley also developed clinical tools to help medical professionals address chronic pain. He developed the Graded Motor Imagery (GMI) treatment, which includes three major psychological techniques:
1. Left/right discrimination training – helps patients in chronic pain restore normal recognition of left and right sides associated with the areas of their chronic pain
2. Motor imagery exercises – a brain exercise when the patient in chronic pain repeats imaginary movements of the affected parts without actual movements
3. Mirror therapy – is a very interesting technique which was originally developed by Dr. V.S. Ramachandran for patients with phantom pains (see Fig. 2).

Fig. 2. Original concept of Mirror Therapy developed by Dr. V.S. Ramachandran
The patient puts the stump (amputated left forearm in Fig. 2) behind the mirror and places a good limb in front of the same mirror. The patient looks into the mirror and now sees both the good limb and its reflection, which seems to indicate that the patient now has both limbs intact. While moving the good limb, he now also sees movements of the lost limb. At this moment, the combined activation of the visual cortex and proprioceptors allows for the temporary elimination of phantom pains in the amputated limb, and with repetitive application, it helps patients manage this debilitating condition.
Prof. Moseley also dedicated his research time to examining a variant of Mirror Therapy called Rubber Hand Illusion (RHI). RHI is also a fascinating technique and let’s go over it with the help of Fig. 3.

Fig. 3. Rubber Hand Illusion
The healthy individual sits with their left hand hidden from view behind the solid screen, and a rubber hand is placed on the table in its place. The other real hand is on the table, but it is separated from the fake one by the screen. If the practitioner simultaneously strokes the fake hand and the real one, the subject will feel similar sensory stimulation in both hands – the real one and the rubber one – despite the fact that the real hand wasn’t stimulated and it is hidden from view.
This simple experiment opens great clinical possibilities. If RHI has such an impact on the brain, it may be possible that, let’s say, the patient with chronic hand pain may get relief from RHI. As it was shown by Prof. Moseley (2005), this is exactly the case. The patients with Complex Regional Pain Syndrome indeed obtained pain relief with Prof. Moseley’s psychological interventions.
Thus, Prof. Moseley deserves considerable credit for his contributions to pain science. However, he works with a special group of patients who have a great central component of pain, like phantom pains or Complex Regional Pain Syndrome. There is no doubt that these techniques are extremely beneficial to those patients. However, this isn’t the case when the patient has chronic pain as a result of various somatic or visceral abnormalities.
Unfortunately for somatic rehabilitation, several ‘educators’ took Prof. Moseley’s work literally and generalized it in all cases of chronic pain, considering that it has only a central component. It completely undermines the basic concept of Gate Control Theory and Neuromatrix Theory, which emphasize the critical role the peripheral component plays in the formation of pain perception. First of all, let us quote Prof. Moseley, since his work is actively cited and misused by proponents of these unscientific ideas, and any counterargument is labeled as “outdated science.” These are quotes from articles Prof. Moseley co-authored:
“…there is limited systematic evidence, and the paradigm (mirror therapy by JMS) appears to be counterproductive during early rehabilitation.” (Giummarra, M., Moseley, L., 2011).
“In two experiments, undertaken by independent research teams and both powered to detect a clinically relevant effect, we failed to detect any modulation of pain thresholds, nor of pain evoked by individually calibrated high and low painful stimuli, in association with the rubber hand illusion.”
and
“This finding suggests against the utility of the rubber hand illusion as a therapeutic tool for pain relief in a clinical setting…” (Mohan R, Jensen KB, Petkova VI, Dey A, Barnsley N, Ingvar M, McAuley JH, Moseley GL, Ehrsson HH., 2012).
Additionally, several studies have analyzed scientific data regarding the clinical application of these techniques and concluded that they do not consistently produce stable clinical results when used as the sole treatment tool in clinical practice.
“There is a moderate quality of evidence that Mirror Therapy as an additional intervention improves recovery of arm function, and a low quality of evidence regarding lower limb function and pain after stroke. The quality of evidence in patients with complex regional pain syndrome and phantom limb pain is also low. Firm conclusions could not be drawn.” (Rothgangel et al., 2011).
“There is presently little evidence describing the value of the rubber hand illusion and virtual hand illusion as indices in the diagnosis or treatment of different pathologies...” (Christ and Reiner, 2014)
So, when should the psychological techniques examined and developed by Prof. Moseley be used? The possibilities are countless: negative body image and loss of body ownership (Lenggenhager et al., 2014), body dysmorphic disorders (Kaplan et al., 2014), robotic hand ownership (Caspar, 2014), etc. It is clear that all of these fields of application are beyond the scope of practice of massage therapy.
Despite modern science proving that treatment based on the central component of chronic pain is a misleading concept, several ‘new” massage methods that are based on the same notion were proposed. For example, Dermatoneuromodulation, which is a combination of well-known medical massage techniques such as nerve stretching and skin mobilization, is often put together and simply renamed as a new modality.
Could techniques advocated by Prof. Moseley be used by somatic practitioners? Absolutely! However, they should be used in combination with correctly designed MEDICAL MASSAGE PROTOCOLs in an integrative concept rather than used alone or as a silver bullet for all cases of chronic pain we as humans experience. We will discuss these topics in the last part of this article in the next issue of JMS.
REFERENCES
Butler, D. S., & Moseley, L. S. (2003). Explain pain. Adelaide: NOI Publications. Dudai, Y. (1989). The neurobiology of memory. Concepts, findings, trends. Oxford: Oxford University Press.
Caspar EA, De Beir A, Magalhaes De Saldanha Da Gama PA, Yernaux F, Cleeremans A, Vanderborght B. (2014) New frontiers in the rubber hand experiment: when a robotic handbecome one’s own. Behav Res Methods.
Christ O, Reiner M. (2014) Perspectives and possible applications of the rubber hand and virtual hand illusion in non-invasive rehabilitation: technological improvements and their consequences. Neurosci Biobehav Rev. Jul, 44:33-44.
Giummarra, M., Moseley, L. (2011), Phantom Limb Pain and Bodily Awareness: current concept and Future Directions., Current Opinion in Anesthesiology 24: 524–531.
Kaplan RA, Enticott PG, Hohwy J, Castle DJ, Rossell SL. (2104) Is body dysmorphic disorder associated with abnormal bodily self-awareness? A study using the rubber hand illusion. PLoS One. Jun 12;9 (6):e99981.
Lenggenhager B, Hilti L, Brugger P. (2014) Disturbed Body Integrity and the “Rubber Foot Illusion”. Neuropsychology. Sep 29.
Melzack R. (1990) Phantom Limbs and The Concept of Neuromatrix. Trend Neurosci.. 13:88-92.
Melzack, R., Katz J. (2013) Pain. Wiley Interdisciplinary Reviews: Cognitive Science, 4(1):1-15, Jan/Feb., 2013
Melzack, R. (2001) Pain and the Neuromatrix in the Brain. J. Dental Ed., 65:1378-1382.
Melzack, R, Loeser J.D. (1978) Phantom Body Pain in Paraplegics: Evidence for Central ‘Pattern Gathering” Mechanism” for Pain. Pain, 4:195-210
Moseley G.L. (2005) Is successful rehabilitation of complex regional pain syndrome due to sustained attention to the affected limb? A randomized clinical trial. Pain. Mar;114(1-2):54-61.
Mohan R, Jensen KB, Petkova VI, Dey A, Barnsley N, Ingvar M, McAuley JH, Moseley GL, Ehrsson HH. (2012) No Pain Relief with the Rubber Hand Illusion. PLoS One. 7(12):e52400.
Rothgangel, A.S.; Braun, S.M.; Beurskens, A.J.; Seitz, R.J.; Wade, D.T. (2011). The clinical aspects of mirror therapy in rehabilitation: a systematic review of the literature. International Journal of Rehabilitation Research 34 (March): 1–13.
Selye, H. (1955). Stress and Disease. Science 122: 625–631.
Category: Medical Massage
