
The purpose of this section of the Journal of Massage Science to inform the practitioners about valuable articles that frequently go unnoticed, as well as to point to those authors and publications who exhibit low educational standards. We do not play politics and we are not associated with any publishing company or professional association. We are a completely independent voice and we promise you direct unbiased reviews based strictly on the science.
If the author of the reviewed article does not agree with our opinion, we will be more than happy to publish his or her response and have a productive discussion over the article’s subject.
At the end of the year we will recognize and reward the author of the most important publication(s) and point to the authors of the most unscientific publication(s). We hope this will help to raise the bar of published materials in massage journals for the benefit of the entire profession.
Massage Today

Just the Facts: Opinion vs. Data in the Therapeutic Relationship. Massage Today, April, 2015, Vol. 15, Issue 04
By Ben Benjamin, PhD
This is a very good article. It emphasizes a critical element of therapy which is very frequently missed – correctly worded communication with the client/patient. Many therapists lack these important skills or don’t use them fully.
The Internet gives the patient a great deal of information even before they see a therapist for the first time. This is why weakly expressed personal opinion by the therapist without solid foundation will be disregarded by the patient. Unfortunately, it has a dual negative impact:
1. The patient won’t follow recommendations to do homework and may well cancel appointments or arrive late for treatment.
2. The therapist loses the healing impact of the ‘placebo effect’ generated in and by the central nervous system as a response to the therapist’s intervention.
Also, the subject raised in this article has another equally important aspect. Incorrectly presented information, which is based on the therapist’s or educator’s personal opinion greatly diminishes the chance that other health practitioners (MD, DO, DC, PT) will express interest in the therapist’s work. The author deserves credit for raising this important topic.
Divide Between Massage Therapists and Energy Bodyworkers: Why? Massage Today, April, 2015, Vol. 15, Issue 04
By Marie-Christine Lochot, LMT
The article examines the divide which currently exists between massage therapists and energy bodyworkers. This topic deserves a separate and longer discussion, but we would like to briefly weigh in on it.
The author is correct when she says that both modalities carry a spiritual component. Yes, Swedish Massage also delivers this since human touch is a critical element in our development and well-being. From the very beginning we were deeply social animals. Look at primates in the zoo and pay attention to how important touch is in the form of grooming or play in their lives.
Development of our children greatly depends on touch interaction with parents, siblings and friends. As we grow we become touch deprived since tactile interaction between humans, especially in the Western world, has become minimal. Often, a hand shake is the most we get from people around us. All other interactions we consider an invasion of our privacy. Such minimal touch interactions are woefully insufficient for normal functioning of our CNS and that contributes to our overall level of stress. This is why even basic Swedish Massage fills this gap.
There is one issue in regard to Reiki and its relation to Swedish Massage which demands clarification. Yes, there are some small sample size studies which examined the benefits of Reiki. Yes, they found that clients feel less stressed after the Reiki session. Since they feel less stress after Swedish Massage as well, the application of Reiki or massage becomes the client’s personal choice.
However, there is one significant difference between Swedish Massage and Reiki. One can learn and master Swedish Massage while one must have some inborn capabilities to successfully practice Reiki. This is a rarely mentioned fact especially by Reiki educators. In other words you can’t learn Reiki but you can greatly enhance it with proper training. Why is that? Each of us has our own bioelectrical field generated by the body. It is composed of electrical impulses generated in the CNS, in the peripheral receptors in the soft tissues and inner organs, by muscle contractions, blood flow, radiation of heat, etc.
For the therapist who practices Reiki to be successful, his or her personal field must be stronger than the client’s. This is a basic rule of Energy Medicine. Let’s say the therapist normally has a low bioenergy field. It isn’t bad for the therapist’s health but it means that his or her performance as a Reiki practitioner is very limited only to those who have an even lower bioelectrical field. To the contrary, the therapist with an inborn strong bioelectrical field has much greater success with practice, especially if his or her inborn capabilities were enhanced by the skillful teacher. There is even a Two Hands Test which allows the therapist to detect if his or her bioelectrical field is stronger than the client’s. If it is not, the application of Reiki becomes as the author correctly mentioned it at the beginning of the article – ‘a sham.’
The Difference Between Adult and Pediatric Massage. Massage Today, April, 2015, Vol. 15, Issue 04
By Tina Allen, LMT, CPMMT, CPMT, CIMT
The author is a great advocate of Pediatric Massage and she deserves a lot of credit for her work. In the past we’ve disagreed with the author on several occasions and published our opinion in previous issues of JMS (see Issues #2, #3, #4, 2014 and #1 and # 2, 2015). In this article the author stated her vision of Pediatric Massage:
“Some healthcare providers only think of Pediatric Massage being applied as a modality for children with special healthcare needs. There are specific healthcare-related situations where Pediatric Massage therapy will be a wonderful part of a therapeutic treatment plan. However, just as adults receive massage therapy for general health and wellness, so do children. Yes, we can use pediatric massage as indicated to treat a variety of healthcare considerations, but dealing with anxiety, stress and insomnia are also concerns for our younger clients.”
We completely agree with this statement. Our previous disagreements were in regard to using stress reduction massage for children with pathological abnormalities. One example is one of the author’s previous articles about Torticollis treatment in young children (see our review in Issue #1, 2015, JMS). Our point was that pathological conditions like Torticollis must be treated with special MEDICAL MASSAGE PROTOCOLs which are based on scientific and clinical data.
As long as the author stays within stress reduction and developmental effects of Pediatric Massage her recommendations should be widely accepted. However, we are sure that the medical application of Pediatric Massage isn’t the place for personal opinion or preferences since it is the child’s health at stake and the treatment recommendations must be carefully measured.
Massage Reduces Non-Specific Shoulder Pain and Improves Function. Massage Today, April, 2015, Vol. 15, Issue 04
By Massage Therapy Foundation
Contributed by Derek R. Austin, PT, DPT, MS, BCTMB, CSCS; Jolie Haun, PhD, EdS, LMT; Pualani Gillespie, LMT, MS, RN, BCTMB
The article informs readers about results of a systemic review with meta-analysis conducted by Van der Dodler, et.al. (2014) of 20 individual trials examining the effects of massage and exercise in patients with non-specific shoulder pain. This article concludes that massage therapy provides various clinical benefits for patients with shoulder pain. Here is quote from the article:
“Based on data from these 20 trials, the authors (Van der Dodler et al., by JMS) conclude that soft tissue massage is effective for improving range of motion function and pain…”
At the end the authors of article in Massage Today made the following conclusions:
“First, this systematic review makes a significant contribution to the body of massage research providing supportive evidence that soft tissue massage is effective for improving range of motion, function and pain in people with shoulder pain. Second, these findings provide practitioners with the evidence needed to justify using massage techniques as an effective means of treatment for shoulder pain and stiffness. Finally, as research accumulates and supports evidence-based practice for treating common conditions such as shoulder pain, the field of massage will increase its presence in the practice of personal health and wellness.”
Reading the article in Massage Today left the impression that the authors of the reviewed meta-analysis study confirmed the clinical effectiveness of massage therapy in the treatment of non-specific shoulder pain. However, the abstract of the article reviewed in Massage Today stated the complete opposite. Here is quote from the abstract:
“There is low-quality evidence that soft tissue massage is effective for improving pain, function and range of motion in patients with shoulder pain in the short term.”
As readers may see, this quote by Dr. Van der Dodler and his co-authors came to a completely opposite conclusion. To find where the truth is we went to the British Journal of Sports Medicine and for $37 bought full access to the article.
Here is what we found. Yes, the authors reviewed 20 studies using meta-analysis and they found that various methods of massage therapy when applied alone (e.g., regular Soft Tissue Massage at the lateral border of scapula, Cyriax’s Cross Fiber Friction, Trigger Point Therapy) produce low-quality evidence that they are effective for improving range of motion, function and pain.
What the authors of the article in Massage Today missed or didn’t mention for some reason is a very interesting fact. Van der Dodler’s study confirmed improvement in the clinical picture of shoulder pain when several modalities were used during the same treatment session – Trigger Point Therapy, deep stroking massage, hold-relax stretch, passive stretching and home exercises mixed together.
This is exactly what the science of Medical Massage recommends. Stable clinical results can be achieved only when several somatic modalities are combined together to rehabilitate affected soft tissues. This can happen only if the therapist has enough tools in his or her tool box and knows how to combine them together for the patient’s benefit.
We think that instead of the authors’ wishful thinking, especially considering that they represent the Massage Therapy Foundation, the authors should analyze and critique the nature of examined studies. We think that their impressive credentials give them this power. For example, how can the study where shoulder pain was treated using only soft tissue massage on the lateral border of the scapula be even considered to be seriously examined? Who treats shoulder pain with working strictly along the lateral scapula? It is almost the same as when an oncologist removes half of the tumor and wonders after that why the patient’s cancer still progresses.
REFERENCES
Van den Dolder PA, Ferreira PH, Refshauge KM. Effectiveness of soft tissue massage and exercise for the treatment of non-specific shoulder pain: a systematic review with meta-analysis. Br J Sports Med. 2014 Aug;48(16):1216-26.
If You Bet the Ranch, You Might Just Lose It. Massage Today, April, 2015, Vol. 15, Issue 04
By Ralph Stephens, BS, LMT, NCTMB
In this article the author illustrates the absurdity of some research (this time in the UK) in the field of manual medicine and massage therapy.
Pes Anserine Tendonitis vs. Medial Meniscal Tear. Massage Today, 2015, Vol. 15, Issue 04
By Debbie Roberts, LMT
A very good and informative article. The title explains its content. The author deserves credit for correctly understanding the rules of massage science. Stable clinical results come from a combination of methods and techniques. Here is a final quote from the article which illustrates the author’s treatment strategy:
“My personal formula is MMT, Myofascial Release with either hands on or cupping to target muscles, heat, PNF, re-test and repeat this formula up to ten times in one hour or until there is relief of symptoms.”
Unfortunately the author is among a minority of therapists since a majority practices one or two modalities they’ve learned. The therapist must adjust treatment strategy to each patient’s needs instead of trying to squeeze them into an incorrect system of personal beliefs.
The Role of Massage Therapy in Dementia Care. Massage Today, April, 2015, Vol. 15, Issue 04
By Ann Catlin, LMT, NCTMB, OTR
A very well written and researched article on the role of massage in the management of dementia. It can be a helpful reference source for those therapists who work with older clients, particularly in special facilities like nursing homes.
The Hallux Valgus and Lower Extremity Dysfunction. Massage Today, May, 2015, Vol. 15,
Issue 05
By Whitney Lowe, LMT
A good article on Hallux Valgus deformation of the foot. It gives a nice review of the problem with proper illustrations. The massage treatment options for Hallux Valgus are presented very modestly and this is the only weak part of the article.

How Often Should You Treat? Massage Today, May, 2015, Vol. 15, Issue 05
By Ralph Stephens, BS, LMT, NCTMB
This article discusses several topics and one is necessary frequency of what the author calls clinical massage. He shares with readers his way of formulating a course of massage therapy, but it is just personal opinions and the author doesn’t provide any reasonable explanation as to why the approach he recommends is the correct one.
The article suggests the therapist should book the first two appointments one week apart. Before the second session starts the therapist should ask the client when his or her symptoms came back. Let’s say that the client told the author that some symptoms came back in four days. Based on that information the author from now on uses a 4-day break between sessions.
So, the client felt the return of pain or other symptoms in four days, but the author sees the client in a week anyway just because his mind was pre-set to one weekly session. In such a case, by seeing the client in seven days instead of four days (as soon as the symptoms returned) the author loses three days of precious time, which he could have used to build a clinical response.
The next question is why the therapist from now on needs to work on the client every four days? Where did that came from? This idea has nothing to do with clinical thinking of effective therapy. Let’s look at how the treatment must be formulated when it is based on clinical science. First of all, the break between sessions is an exceptionally important clinical tool which the therapist must master if he or she would like to be effective.
Before you start your first session ask the patient to concentrate and remember the intensity of uncomfortable sensations before treatment begins. The following session should be scheduled with a one day break if the initial symptoms were mild to moderate. If the patient was in a lot of pain to start with, the next session must be scheduled on the day any new sensations which appeared after the first session are gone. It may take 2 or in the worst scenario 3 days. Every extra day the therapist waits and the patient isn’t treated works against the treatment plan and the patient. While pushing forward the breaks become shorter.
This is a general outline of Medical Massage framework which is currently used in every medical facility where this modality is employed. The approach recommended in the article greatly lengthens the course of the therapy since it doesn’t allow the therapist to build up clinical response because the breaks between sessions are too long.
The author mentions that Russian Medical Massage schools “…utilize 15 to 20 minute sessions, several times a week.” First of all, there is no such thing as Russian Medical Massage. This is a complete misunderstanding of the Medical Massage concept. The modern school of Medical Massage is a result of the international cooperation of scientists and clinicians from many Western countries. Here is a basic list of countries arranged in chronological order: Russia, Austria, Germany, France, USA.
Secondly, Medical Massage requires a maximum of three sessions per week and they must be at least 30 minutes long. Each minute of a treatment session carries a specific goal and targets various soft tissue structures with a special set of techniques.
We fully agree with this statement:
“…therapists are destroying their bodies doing “Deep Tissue Massage.”
Multi-Layered Therapy. Massage Today, May, 2015, Vol. 15, Issue 05
By Debbie Roberts, LMT
The article in easy to read and its understandable format describes the concept of General Adaptation Syndrome (GAS) developed by French scientist Prof. Hans Selye, The article also emphasizes the importance of using all the therapist’s sensory tools to evaluate and work on the client.
Fascial Health with Vacuum Therapies. Massage Today, May, 2015, Vol. 15, Issue 05
By William F. Burton Jr., LMT, CMCE
We completely agree with the main point of this article that cupping (especially mobile cupping) is an effective clinical tool to decrease tension in fascia. The article itself is a very weak piece.
Listening to Your Clients. The importance of reflection in therapeutic communication. Massage Today, June, 2015, Vol. 15, Issue 06
By Ben Benjamin, PhD
The subject of this article is communication with the client before treatment starts. It is an issue of great importance. Unfortunately, the article doesn’t deliver the contents that match its topic.
Massage Therapy Can Reduce Inflammation at the Circulatory Level. Massage Today, June, 2015, Vol. 15, Issue 06
By Massage Therapy Foundation Contributor
Contributed by MK Brennan, MS, RN, LMBT; Derek Austin, PT, DPT, MS, BCTMB, CSCS and April V Neufeld, BS, LMP
A good source of scientific data on how massage helps recovery after strenuous exercises. It can be used by therapists to justify what they are doing. We also discussed this issue in articles: ‘United We Stand’ Issue #5 2009 and ‘Response To New York Times Interview With Prof. M. Tschakovsky’ in Issue #5 2010.
The Strain of Compression. Massage Today, June, 2015, Vol. 15, Issue 06
By Dale G. Alexander, LMT, MA, PhD
This is a very good article which proves the author can write good educational pieces when he avoids personal opinions filled with unscientific claims. We greatly agree with the statement that:
“…soft tissues serve the joints. It is nature’s hierarchy. Much of any excessive tension around and between the joints is created because the joint surfaces become stuck in mid-range, prevented from completing their full range of motion and thus are structurally misaligned in their proper tracking relationships.”
Tissue Density Palpation. Massage Today, June, 2015, Vol. 15, Issue 06
By Linda LePelley, RN, NMT
A very basic article on soft tissue palpation.
Massage & Bodywork Magazine
Always On. Massage & Bodywork Magazine, March/April, 2015: 26-27
By Douglas Nelson
A very good clinical case report.
Platysma. Massage & Bodywork Magazine, March/April, 2015: 43-44
By Christy Cael
A good article on the anatomy, function and palpation of the platysma muscle.
Massage Therapy Eases Fibromyalgia. Anxiety, Depression and Pain are Reduced. Massage & Bodywork Magazine, March/April, 2015: 46-49
By Jerrylin Cambron
A very informative source on the effect of massage on patients with Fibromyalgia.
Groin Pulls. Adductor Longus Strain and the Iliopsoas. Massage & Bodywork Magazine, March/April, 2015: 90-95
By Whitney Lowe
A very good and informative article on adductors and iliopsoas injury.
Text Neck and Desktop Neck. Massage & Bodywork Magazine, March/April, 2015: 90-95
By Erik Dalton
A great article on pain pattern associated with overloading of the posterior cervical muscles.
Working with the Mesentery. Massage & Bodywork Magazine, March/April, 2015: 90-95
By Til Luchau
A very good article on working with mesentery. The technique which is described in this article is part of Visceral Manipulation Therapy. To our great surprise we read the following statement:
“…the technique (i.e. Mesentery Technique by JMS) applied here is not Visceral Manipulation Therapy, the method developed by French osteopath Jean-Pieree Barral.”
No one disputes the importance of Dr. Barral’s work but Mesentery Technique described in the article wasn’t developed by him or by Mr. Til Luchau. It is as old as Visceral Manipulation Therapy itself. Dr. Barral can be credited only with introducing it to American therapists.
For example, the Editor in Chief of our Journal learned this technique in medical school in the 1980s when it had already been taught for decades. Thus the author is incorrect in this matter since Mesentery Technique is indeed part of Visceral Manipulation Therapy.
Always On. Massage & Bodywork Magazine, May/June: 26-27, 2015.
By Douglas Nelson
There is much less practical information in this case report. We should emphasize the fact that in many cases correct observation of the patient as soon as he or she enters the room gives the therapist a lot of helpful clues. This is exactly what the author did. We addressed this issue separately in our article, ‘Science of Visual Evaluation’, in issue #2, 2015 of JMS.
Supinator. Always On. Massage & Bodywork Magazine, May/June: 41-42, 2015.
By Christy Cael
This article correctly presents anatomy, function and especially palpation of the supinator muscle. The supinator muscle is the deep muscle of the dorsal forearm and it is located under brachioradialis and extensor digitorum communis muscles.
Many times we emphasized in our reviews that while correctly presenting palpation of the specifically located muscles, the author frequently made mistakes when describing palpation of the deep muscles. In this article she got everything right. Indeed to palpate the supinator muscle the therapist must move superficially located muscles to the side instead of palpating through them.
Studies Show Effectiveness of Massage for Addressing Nonspecific Low-Back Pain.
Massage & Bodywork Magazine, May/June: 44-47, 2015
By Jerrilyn Cambron
This article reports on results of a study where Swedish Massage was tested in the clinical setting against physical therapy in cases of lower back pain. The authors found more clinical benefits in the group which received Swedish Massage. The good thing about this study is that if even basic Swedish Massage gave better clinical results, the application of correctly formulated MEDICAL MASSAGE PROTOCOL will give even more impressive and stable clinical results.
Fascia-Related Dysfunction Palpation and Functional Assessment Methods. Massage & Bodywork Magazine, May/June: 64-71, 2015
By Leon Chaitow
A great article on fascia, its function and role in the development of soft tissue pathologies.
Massage and the Indirect Approach to Nerve Injury. Massage & Bodywork Magazine, May/June: 91-97, 2015
By Whitney Lowe
Overall this is a good article which correctly describes the pathophysiology of ulnar nerve compression, its testing and treatment strategies. However, there are statements we greatly disagree with. They show that the author doesn’t have a full understanding of the basic aspects of clinical massage when nerve injury is present. Here is an example quote:
“If the nerve roots are involved, there is little that massage can do to address it, because structures are too deep. In addition, massage can’t do anything to the nerve directly to help it heal.”
These statements are complete nonsense. Medical Massage is the first line of defense for cases when nerve roots are irritated or compressed by the intervertebral disks. If this modality fails, the other treatment options like injections or surgery should be considered. More likely while readers read this review, patients with nerve roots pathologies are treated in clinics in Phoenix, Los Angeles, San Antonio and Daytona Beach, all of which are associated with the Science Of Massage Institute.
Also there are direct and indirect treatment options which help the nerve to heal. We are sure that the author doesn’t have the professional right to make these ungrounded statements since they do not promote learning and practicing Medical Massage by a therapist who may otherwise bring great relief to these patients.
Myoskeletal Enhancers.Engaging the Brain, Freeing the Fascia. Massage & Bodywork Magazine, May/June: 99-100, 2015
By Erik Dalton
A good article which informs readers on the techniques the author used to heal a patient with cervical pain and restriction. We would like to emphasize one important point that should not be missed. The author treated the patient for three weeks and used other treatment strategies as well. Thus we don’t want readers to think that what is discussed in the article is only what should be used.
Working with Clients’ Locked Knees. Massage & Bodywork Magazine, May/June: 106-109, 2015
By Bethany Ward and Til Luchau
This article describes knee hyperextension or genu recurvatum, its causes, pathophysiology and treatment options. Sometimes reviewing articles in massage publications is a very sad process. It amazes us how much disinformation and unscientific claims are published and how much they mislead therapists. This article is an unfortunate example of this sad tendency. Almost everything in the article is incorrect or incorrectly presented.
1. PATHOLOGY ITSELF
Within the healthy population of teenagers and young adults knee hyperextension or genu recurvtum (in Latin) is due to inborn joint laxity as is correctly mentioned in this article. This extra-elasticity of soft tissues around the knee joint will disappear with age without any intervention. Only the individuals who exhibit a negative tendency of deformation increase require intervention.
At the same time, knee hyperextension can be a sign of some very complex medical conditions. In these cases Genu recurvatum always is the result of structural changes inside the knee due to internal mechanical damage – menisci, ACL, PCL, etc. Also, knee hyperextension can develop as a result of stroke, polio, cerebral palsy or various motor deficits.
The authors try to justify the necessity of treatment of knee hyperextension among an otherwise healthy population through several references. Here are their titles:
1. “Effect of Genu Recurvatum on the Anterior Cruciate Ligament-Deficient Knee During Gait”
2. “The Relationship Between Static Posture and ACL Injury in Female Athletes”
3. “Correction of Genu Recurvatum Secondary to Osgood-Schlatter Disease: A Case
Report”
As readers can see in all references used in the article, their authors examined hyperextended knees after mechanical trauma or disease (underlined parts of the titles). Thus the necessity of knee hyperextension’s correction for young healthy individuals recommended in the article is completely baseless since the references from the article emphasized the development of genu recurvatum secondary. In such cases the original trigger must be treated first and the article’s recommendations become waste of time.
2. PATHOPHYSIOLOGY
Let’s drop cases of those young individuals whose genu recurvatum is the result of inborn laxity of the soft tissues. Here are three pathological mechanisms of genu recurvatum accepted by modern medicine:
1. External rotary deformity
As a result of neurological pathologies (e.g., cerebral palsy, stroke, etc.) the patient starts to walk with the forefoot in inner rotation and extension in the ankle joint.
2. Internal rotary deformity
As a result of the same conditions the patient starts to walk with the forefoot in outer rotation.
3. Non-rotary deformity
In these patients the foot and ankle are in normal position and the genu recurvatum is the result of the knee pathology itself. The main cause of non-rotary deformity is knee trauma (ACL, menisci, etc.). Only a very small number of patients may have non-rotary genu recurvatum as a result of muscle disbalance. There is great chance that a therapist will never see those patients during his/her professional career.
This article leaves the impression that genu recurvatum is a very common pathology and it can be successfully treated by the technique discussed in the article. This is absurd since massage therapy is unable to make any stable clinical improvements for patients with external, internal and non-rotary (as a result of trauma) deformities. It doesn’t matter what article proclaims, but while these patients may feel generally better after the therapy there is zero chance to reverse genu recurvatum since the knee hyperextension is a secondary issue. To correct genu recurvatum the original pathology must be addressed first.
3. TREATMENT
The treatment section of the article correctly mentions the necessity of a comprehensive approach to knee rehabilitation. Since in a great majority of cases the genu recurvatum is a consequence of various medical conditions where any massage treatment of the knee is useless without its original trigger being first corrected by surgery or various braces, orthotics etc. (Fish and Kosta, 1998.)
What is really puzzling is the myofascial technique recommended in the article as a tool to treat genu recurvatum as a result of muscle disbalance or locked knee. To illustrate our point we will use the same diagram from www.somastruct.com which the authors used in their article. Fig. 1 shows a lateral view of a normal and hyperextened knee.
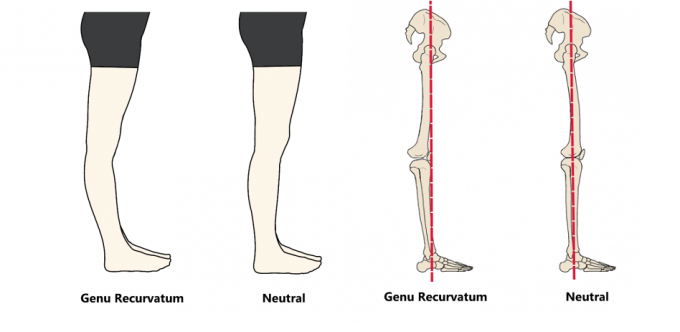
Fig. 1. Normal and hyperextended knee
Here is quote from the article which describes the nature of the recommended technique:
“This technique is an excellent approach for releasing any fascial inelasticity and shortness in front of the leg that can contribute to knee locking.”
So the idea of the treatment recommended in the article is to reduce tension and shortening of the quadriceps muscle. On first glance this is an excellent idea since the lateral view illustrates that the hamstring muscles are supposed to be overstretched and weak, while the quadriceps must be shortened and tense (see Fig. 1).
However, the clinical reality is much more complex than its understanding by the authors. In those who developed genu recurvatum as a result of muscle disbalance, the pathological chain of events starts in a completely different part of the body far from the anterior knee the authors are trying to treat. The weakening of the gluteal group is the first step in the development of genu recurvatum. Let’s put everything in motion (Zeiler, 2011):
1. Overload of the gluteus maximus during intense physical activity shortens its fibers and the muscle becomes weaker. The weaker gluteus maximus muscle delays initiation of contraction and makes it less efficient. Thus during physical activity with every step the individual takes there is a delay in gluteus maximus contraction.
2. Gluteus maximus and hamstring muscles are prime movers for hip extension especially during physical activity. For the lower back and entire lower extremity to work correctly, the gluteus maximus muscle needs to fire first before the hamstring muscles to support efficient hip extension. If the gluteus maximus fails to initiate this action, the hamstring muscles start to work harder.
3. To fight with exhaustion, the hamstring muscles greatly increase their tension. This is the driving force of knee hyperextension since these muscles insert on the posterior surface of the tibia and fibula and they pull the posterior knee backward. As a following change, tension develops in the gastrocnemius muscle which reinforces genu recurvatum.
4. Spasm in the hamstring and gastrocnemius muscles also makes the quadriceps weaker.
Without understanding the nature of genu recurvatum, the authors recommend concentrating on and reducing tension in the quadriceps muscle, which is already weaker! At the same time they don’t even mention the critical importance of working on the gluteus maximus, hamstring and gastrocnemius muscles first. Only after the therapist works on all of them should the quadriceps be worked on, but with completely opposite stimulating massage techniques!
The absolute lack of understanding of the topic the authors are trying to cover is very surprising since even basic research of medical sources on the Internet is widely available. Unfortunately, checking the validity of their own ideas apparently wasn’t the authors’ priority.
Here are a couple of articles which completely destroy their theory:
Loudon, et al., (1998) stated that weakness (not tension as is suggested in the article by JMS) of the quadriceps muscle should be addressed.
Devan et al., (2004) showed that changes in Hamstring:Quadriceps ratio is the main cause of knee overuse and formation of genu recurcatum in athletes. According to the authors, addressing hamstring muscles is a major treatment priority.
We would like to inform readers that for this review we conducted intensive research in medical literature and didn’t find even a distant mention that reducing tension in the quadriceps will reverse genu recurvatum. Several times already we’ve caught Mr. Luchau manipulating scientific sources for the benefit of his incorrect views and this article is another unfortunate example (see our reviews of Mr. Luchau’s articles, which touch on the author’s manipulation of scientific data: on Headache Treatment in the Nov/Dec Issue 2010; on evaluation of sciatic nerve entrapment in Issue #4 2011; and on the treatment of Vertigo in Issue #2 2014).
REFERENCES
Devan MR, Pescatello LS, Faghri P, Anderson J. A Prospective Study of Overuse Knee Injuries Among Female Athletes With Muscle Imbalances and Structural Abnormalities. J Athl Train. 2004 Sep;39(3):263-267.
Fish D.J, Kosta C.S. Genu Recurvatum: Identification of Three Distinct Mechanical Profiles. JPO, 1998 10(2): 26-32
Zeiler A. Knee Hyperextension Syndrome. Forward Thinking PT , 2011
Loudon, J.K, Goist H., Loudon, K.L. Genu Recurvatum Syndrome. JOSPT, 1998, 27(5), May 361-367
Massage Magazine
Osteoarthritis. Massage Magazine 228, May: 42-45 2015
By Heath and Nicole Reed
This is a very basic article about Osteoarthritis and the application of massage therapy for pain and stiffness relief. The article provides some reference resources but what it misses is real treatment options. Swedish Massage gives some benefits but MEDICAL MASSAGE PROTOCOLs and their cornerstone Periostal Massage are absolutely unique and powerful treatment tools.
In early stages of Osteoarthritis the regular application of Medical Massage freezes further development of pathologies and together with other modalities (e.g., light exercise, food supplements, etc.) helps patients avoid surgery.
When joint replacement is unavoidable, Medical Massage is helpful in preparing the joint for the surgery and what is more important, it greatly speeds up the rehabilitation process.
Category: Good Apples, Bad Apples
