
Recently we had a 65 year-old female patient who was suffering from burning pain on the lateral aspect of the left foot for almost two weeks. She went to a podiatrist who diagnosed her with Morton’s Neuroma between the 4th and 5th metatarsal bones. The podiatrist gave her a steroid injection which didn’t help her at all. She also indicated she has suffered from chronic sciatic pain on and off for years.
During the examination of her foot she indeed showed signs of Sciatic Nerve Neuralgia which mostly affected the common peroneal division of the sciatic nerve (The Sensory Test was positive; there where changes in the local temperature of the foot, etc.). As for any patient who is treated in our Medical Massage clinic, we examined the affected and neighboring dermatomes all the way to the pelvis. What we found on her sacrum is shown in Fig. 1.
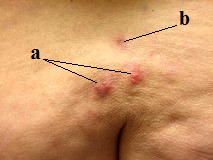
Fig. 1. Skin lesions on the sacrum
a – active lesions
b – scar from previous lesions
What you see in Fig. 1 are skin lesions associated with chronic Herpes Virus infection in the stage of re-activation within the L5 dermatome – the same dermatome which goes all way to the lateral and top of the foot (see Fig. 3). The Herpes Virus is the same agent that causes Shingles. As you can see on the picture, our patient had two reactivation foci and one scar which is visible above the acute lesions. Active lesions look like small bubbles (vesicles) filled with water. The scars after reoccurred infections in the same place look like a dark pigmentation. This how all lesions look like when the patient is in remission.
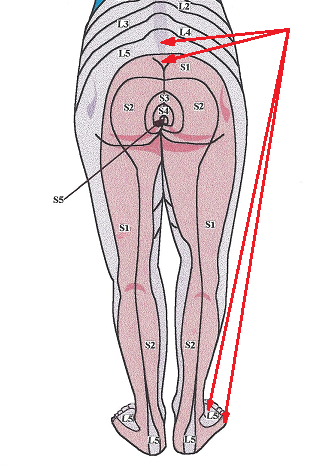
Fig. 2. Map of dermatomes
Red arrows – L5-S1 dermatomes
When we asked the patient about her skin lesions, she said she had them for years and they come and go. When they’re really bad she takes medication, but these didn’t bother her. Here is the clinical situation: the patient had a chronic herpes infection and no one informed her that since the virus lives in the nerves, her coming and going symptoms of sciatica pain were a direct result of a low grade chronic viral infection. In such case any therapy is a waste of time, effort and the patient’s money. The only solution is anti-viral medications. This is what we explained and recommended to her.
Somatic therapists frequently encounter similar situations without being aware of them. Here is the common scenario: If the patient has a low-grade chronic herpes infection he or she will complain about pain in the parts of the body (sometimes distant ones) which are innervated by the affected nerves. In our patient it was the lateral aspect of the foot, but she didn’t have pain in the lower back and no one checked it.
Another problem is that pain starts at least a week, sometimes two weeks, BEFORE the lesions appear on the skin. All this time patients are treated for varieties of somatic pain while the real cause is re-activated viral infection. In such cases the nerve is already inflamed by the multiplication of the virus. However, the viral load isn’t large enough to let the virus spread along the nerve all way to the skin it innervates to create actual skin lesions.
How do you know or suspect the viral infection as a possible cause of somatic pain? There are some direct and indirect clues.
Indirect clues:
1. Usually these are older patients
2. The first couple of sessions don’t bring ANY relief
3. Pain has a burning character (only inflammation of the nerve creates burning type pain)
Direct clues:
1. The patients know (if they asked) hat they have chronic viral infection
2. Usually the Herpes Virus attacks the same areas of the skin and it leaves visible scars in the form of dark pigmentations. If the therapist sees such scars and indirect clues are present, there is a great chance the pain is caused by the virus, but it hasn’t shown as skin lesions yet.
Fig. 3 illustrates the scars on the skin of the right gluteal area (dark pigmentation spots) in one of our other patients who had repeated reoccurrence of the viral attacks there and at the same time suffered from the chronic sciatic-like pains.

Fig. 3. Scars on the right gluteal area after chronic low grade attacks of the Herpes Virus
Generally speaking, the Herpes Virus is mildly contagious and it can be transmittable only if a person has a weakened immune system and he or she comes in direct contact with fluid from the vesicles. The therapist will never become infected if he or she works in the parts of the body where scars are present.
Dr. Ross Turchaninov
LESSONS:
1. A chronic low grade Herpes Virus infection may trigger somatic pain in the areas of lesions or in distant parts of the body.
2. There are no skin lesions for almost two weeks before they appear, but all this time the somatic pain is present.
3. Use indirect and direct clues to consider the possibility of Herpes Virus infection as a trigger for the somatic pain felt by the patient. Verbalize your thoughts to the patient.
4. Don’t treat a patient with acute lesions.
5. While evaluating a patient with any somatic pain, always check the skin along the affected dermatomes using the map of dermatomes as a guide.
Category: Blog
