
The purpose of this section of the Journal of Massage Science to inform the practitioners about valuable articles that frequently go unnoticed, as well as to point to those authors and publications who exhibit low educational standards. We do not play politics and we are not associated with any publishing company or professional association. We are a completely independent voice and we promise you direct unbiased reviews based strictly on the science.
If the author of the reviewed article does not agree with our opinion, we will be more than happy to publish his or her response and have a productive discussion over the article’s subject.
At the end of the year we will recognize and reward the author of the most important publication(s) and point to the authors of the most unscientific publication(s). We hope this will help to raise the bar of published materials in massage journals for the benefit of the entire profession.
MASSAGE & BODYWORK MAGAZINE

The Loudest Voice Wins. Massage&Bodywork Magazine, Jan/Feb: 30-31 2018
By Douglas Nelson
While this looks like a very simple and unimportant article, clinically speaking the author illustrates a very important issue. Very frequently successful treatment of original symptoms the patient came in with coincides with the appearance of new symptoms that look like completely unrelated parts of the body.
The author is completely correct when he explains in this piece an important clinical observation: the decrease of intensity of the original symptoms will make symptoms which were hiding behind the original ones clinically prominent. This scenario confuses patients since they may think that despite improvements the treatment triggered new symptoms. In reality the author has correctly labeled it: The Loudest Voice Wins.
Common Side Effects of a Common Drug. Massage&Bodywork Magazine, Jan/Feb: 40-43, 2018
By Ruth Werner
This article raises a very important topic for therapists and we observe it daily in our clinic and clinics associated with SOMI. Patients who take statins regularly complained about various musculoskeletal syndromes. Therapists should be aware of it since their therapy may fail because the initial trigger in satins is still in the body.
Force Distribution in the Foot. Massage&Bodywork Magazine, Jan/Feb: 44-45, 2018
By Christy Cael
A small but very good article which covers biomechanics of the foot.
The Posture Window. Using Posture to Guide Assessment and Treatment. Massage&Bodywork Magazine, Jan/Feb: 68-75, 2018
By Yoni Whitten, DC
The article raises a lot of important points which can be summarized in a way that Postural Changes are responsible for patients’ pain and discomfort and working on the soft tissues while postural changes are not addressed greatly diminishes the clinical effectiveness of MT.
Yes, the author is correct here, but only in a minority of clinical cases. Based on our clinics combined experience it is approximately 20%. Thus, postural changes may trigger symptoms the author mentioned. However, in a majority of cases the postural changes develop by the brain and secondary reaction to the chronic pain. In such cases addressing the postural changes themselves also becomes a waste of time and effort since the initial trigger must be identified and eliminated first before postural changes should even be considered.
Exploring the Dorsal Scapular Nerve. Massage&Bodywork Magazine, Jan/Feb: 88-91, 2018
By Whitney Lowe, LMT
Great article!
Release the Parking Brake and See What’s Driving the Muscle Spasm. Massage&Bodywork Magazine, Jan/Feb: 92-93, 2018
By Erik Dalton, PhD
Good article.
Squamous Cell Carcinoma. More Than Meets the Eye. Massage&Bodywork Magazine, Mar/Apr: 42-45, 2018
By Ruth Werner
The topic of this article is very important but the article itself misses vital information. Squamous Cell Carcinoma (SCC) is relatively aggressive skin cancer which must be diagnosed asap. It allows the dermatologist to achieve quick and stable clinical results. The article is dedicated to this topic and the author is correct when she states that:
“Massage therapists have a unique privilege: we see more of our clients’ skin (especially on the posterior surface of the body) than they do themselves, and with regular clients, we see that skin over the course of time.”
However, nowhere in the article does the author actually show to therapists a picture of what the early stages of SCC look like. If the article doesn’t provide a correct image of SCC, the entire goal is diminished to the level of basic info without ANY clinical significance. This is the weakest part of the article. Considering the importance of the subject the author raised, but didn’t follow through with, we decided to fill the informational gap in the article and show a picture of the early stages of SCC.

Fig. 1. SCC in early stages
Intervertebral Disks. Massage&Bodywork Magazine, Mar/Apr: 47-48, 2018
By Christy Cael
A very good introductory article on intervertebral disks.
De-Rotators and Other Muscles That Change Their Joint Actions. Massage&Bodywork Magazine, Mar/Apr: 82-89, 2018
By Joseph E. Muscolino, DC
Simply EXCELLENT article!
Guyon’s Canal Syndrome. Massage&Bodywork Magazine, Mar/Apr: 94-97, 2018
By Whitney Lowe, LMT
A very good article on a rarely mentioned subject.
MASSAGE TODAY
Understanding the Gamma Efferent System. Massage Today. 18(1), 2018
By Whitney Lowe, LMT
A very good article!
Restoring Vagal Tone: Improving Your Clients’ Quality of Life. Massage Today. 18(1), 2018
By Dale G. Alexander, LMT, MA, PhD and Michael Shea, PhD
This article covers the important subject of balance in activity of the autonomic nervous system, specifically the increase in the parasympathetic or vagal tone. This subject is especially important in light of new convincing evidences that the body doesn’t have sacral parasympathetic division as we all previously thought.
We have only one concern – that the article heavily relies on the Polyvagal Theory proposed by S.W. Porges, PhD. This theory is definitely ‘food for thought’ and a great point to start discussion, but at the same time it is just theory based mostly on circumstantial evidence. However, we agree with the authors that extending learning including Polyvagal Theory will widen therapists’ intellectual horizons.

Could Massage Spread Cancer in the Newly Diagnosed? Massage Today. 18(1), 2018
By Tracy Walton, LMT, MS
To read the review please click here: https://www.scienceofmassage.com/2018/05/response-to-new-critique-by-t-walton-published-in-massage-today/
TMJ: A Case Study, Treating Beyond the “Dental Approach.” Massage Today. 18(2), 2018
By Don McCann, MA, LMT, LMHC, CSET
The author is completely correct when he states that the dental only approach won’t be able to deliver stable clinical results for patients with TMJ Dysfunction. However, he is mistaken again when he discusses the treatment options.
Mr. McCann considered various biomechanical changes in his patient with TMJ dysfunction as indicators of the tension inside of TMJ built up as a result of pelvis rotation, chest twist, shoulder elevation etc. Clinically speaking the author puts the chicken before the egg since all these biomechanical abnormalities in a majority of cases are secondary developments triggered by the brain as a reaction to chronic nociception stimuli which bombarded his patient’s brain for some time.
Why in such case did Mr. McCan’s treatment work and he was able to help his patient with TMJ Dysfunction? As the author reported in this case study his patient also suffered from chronic headache. In such case the trigger for headache and TMJ dysfunction was more likely mild irritation of the minor occipital nerve by the posterior cervical, scalene and sternocleidomastoid muscles. Here is a quote from the article where the author describes his treatment routine during the first session:
“The first myofascial soft tissue protocol was applied to bring the shoulders and neck back, release the scalenes and sternocleidomastoid so the neck could straighten, and release the back of the neck down to the shoulders so they could drop and balance.”
We bet that this treatment was a key to the author’s success since we observed almost identical response from our patients to similar therapy for patients with TMJ dysfunction triggered by Minor Occipital Nerve Neuralgia. Freeing the minor occipital nerve will deliver quick results and addressing pelvis and chest (as the author did during following sessions) targeted secondary biomechanical and postural syndromes which in many cases will fade away by themselves if headache and TMJ pain are not factors anymore.
So, without fully understanding what did actually happen to the patient, the author used initially correct treatment strategy which had nothing to do with his views of the necessity of addressing secondary symptoms as the main treatment option.
Readers may have a reasonable question: What is the difference? The author helped the patient, and this is what counts.
Working with TMJ patients on daily basis we are sure that correct evaluation is the key to the correct treatment option. The author made a mistake in evaluation, but ironically used the correct treatment option. However, it can’t always be the case since identifying the initial trigger of the somatic abnormality is the foundation of 100% effective somatic rehabilitation.
Meet the Popliteus: A Cause for Knee Pain. Massage Today. 18(2), 2018
By Stacey Thomas, LMT, FMS, SFMA, NKT, CF-L2
We think that for the MT to be fully accepted as a legitimate part of somatic rehabilitation and become part of medicine we all should agree on at least some basics. If there is no unified vision on simple things how can therapists present their case to other health practitioners? There is no way in any other part of medicine one can find completely different pieces of information regarding the same topic. We regularly observe this phenomenon among authors and educators who are addressing the clinical aspects of MT. This article is great example of such an unfortunate trend.
The article is dedicated to the role of the popliteal muscle in the generation of knee pain. Here are three aspects which are erroneously presented in the article:
1. Let’s start with action mentioned in the article for the popliteus muscle:
- Knee flexion
- Lateral rotation of the femur
- Medial rotation of the tibia/fibia
We can produce other sources which will show that the author is incorrect, but let’s use Dr. Travel and Dr. Simmons Trigger Point Manual (1983) as it is widely used and respected by therapists and other health practitioners. Here is a quote from the book from pages 342-343:
“The popliteus muscle is at mechanical disadvantage for producing knee flexion by virtue of the angulation of its fibers and their proximity to the axis of rotation of the knee.”
Both authors also cited several studies which examined the popliteus muscle using electromyography and all authors found that the muscle first of all produces medial rotation of the leg. Its participation in the knee flexion is minimal. Unlocking the knee joint from extension, which the author mentioned in the article, happened first of all because of lateral rotation of the femur during weight bearing (Travel and Simmons, 1983). Thus, the popliteus muscle very weakly supports knee flexion mentioned in the article in the first position while its main action is medial rotation of the leg.
2. The article mentioned tension in the popliteus muscle as an independent pain syndrome. In reality this is not the case. Isolated tension in the popliteus muscle is a very rare event and in the majority of clinical cases pain in the popliteus muscle is due to the mild irritation of the tibial nerve which supplies the popliteus muscle as well as other leg muscles. Here are Travel and Simmons again:
“…popliteus rotates distal part of the limb and seldom presents as a single-muscle myofascial syndrome.”
3. Pain location mentioned in the article is completely wrong. Here is a quote from the article:
“If they’re complaining of pain on the medial and/or front of the knee, especially when they run, walk up stairs, or downhill, those are also signs that palpating the popliteal fossa is a good idea.”
Let’s look at Fig. 2 (Fig. 17-1 from Travel and Simmons, 1983) which indicates a pain pattern generated by the tension in the popliteus muscle.
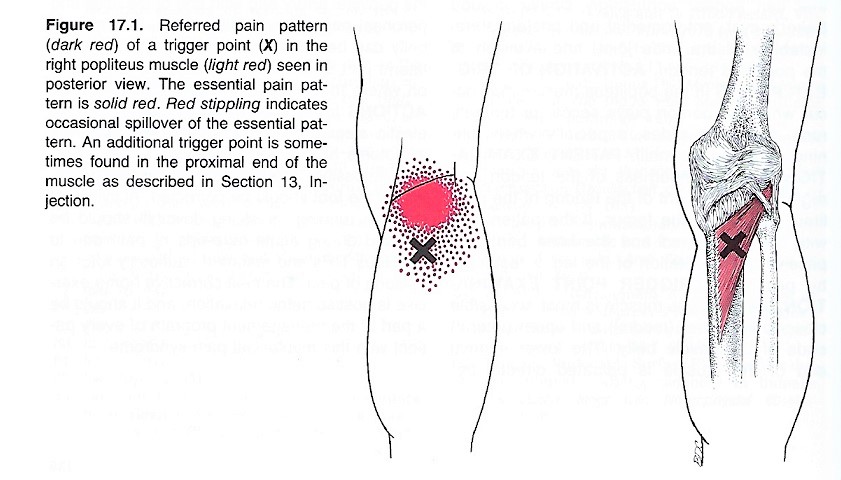
Fig. 2. Referred pain pattern of a trigger point (X mark) in the right popliteus muscle
We ask readers to match the information in the picture with the quote from the article which indicates that the patient with tension in the popliteus muscle will exhibit pain on the “medial and/or front of the knee” as the author suggests.
Let’s for the sake of discussion consider that the author will make the point that Travel and Simmons’ textbook is an old publication. Let’s look at the same topic in recent medical literature.
Chang et al., (2016) used Ultrasonography to examine as they put it, “Uncommon cause of posterior knee pain (bold by JMS)” generated by a tensed popliteus muscle.
Cho et al., (2016) reported a very rare case of the tibial nerve compression by an enlarged popliteus muscle with all symptoms located on the posterior (bold by JMS) knee and leg.
As readers may see, the article provides completely misleading information about the nature of tension in the popliteus muscle but what is more important, it misleads therapists in evaluation and eventually treatment opinions since if the evaluation is done incorrectly the therapist will make treatment mistakes.
What is really upsetting is such low writing standards exhibited by the author who addressed the clinical issue with erroneous assumptions and didn’t even bother to do some basic Google search before writing a piece for a national publication on a clinical subject.
If we can’t agree on such basics where pain in case of the tension in popliteus muscle is located, who in the medical profession will listen to our pleas about the clinical effectiveness of MT?
REFERENCES
Chang KV, Hsiao MY, Hung CY, Özçakar L. An Uncommon Cause of Posterior Knee Pain: Diagnosis and Injection for Popliteus Strain Using Ultrasonography. Pain Med. 2016 Apr;17(4):795-6.
Cho KJ, Kang S, Ko S, Baek J, Kim Y, Park NK. Neurovascular Compression Caused by Popliteus Muscle Enlargement Without Discrete Trauma. Ann Rehabil Med. 2016 Jun;40(3):545-50
Travel J.G., Simmons D.G. Myofascial Pain and Dysfunction. The trigger Point Manual. Williams&Wilkins, 1983
Muscles & Tendons of the Thumb. Massage Today. 18(2), 2018
By Ben Benjamin, PhD
A good article on the anatomy of thumb muscles
Scapulohumeral Rhythm: Looking Beyond the Glenohumeral Joint. Massage Today. 18(3), 2018
By Whitney Lowe, LMT
Very informative article on coordinated movements between the scapula and shoulder joint.
Lymphatic Balancing: The Six-Step Treatment Approach. Massage Today. 18(3), 2018
By Kerry D’Ambrogio, DOM, AP, PT, DO-MTP
The author is completely correct when he emphasizes the frequently overlooked issue of Lymph Drainage Massage not only being helpful in the cases of edema, but it must be a component of every clinical application of MT. LDM is indeed the structural component of each Medical Massage Session.
MASSAGE MAGAZINE
Massage Treatment Planning for the Diabetic Client. Massage Magazine, issue 261: 36-42, Feb, 2018
By Julie Goodwin, LMT
This is very introductory article on Diabetes, indications and contraindications for MT applied for the diabetic patient.
Neural Manipulations. Massage Magazine, issue 261: 48-50, Feb, 2018
By Judy Russell, RMT
This article is on an important clinical subject but the piece itself gives extremely limited information for readers. At least some general outlines or examples would be excellent additions. Without them the article has very limited practical value.
Lymphatic Liquefaction Using Vacuum Cups. Massage Magazine, issue 262: 50-53, Feb, 2018
By Anita Shannon, LMT
This article is a rare piece on the correct application of vacuum as part of rehabilitation.
Category: Good Apples, Bad Apples
Tags: 2018 Issue #1
