
By Dr. Ross Turchaninov
To begin with, I would like to state the article you are about to read is the author’s personal opinion, which is based on clinical experience and detailed research of modern scientific sources. It is also an invitation for further discussion.
Let’s look at some statistical data first. Lehrich et al., 2006 estimated that 80% of people who live in Western countries at least once in their lives suffered severe lower back pain. In the USA alone the combined direct and indirect cost of lower back pain treatment varies between 50 and 100 billion dollars annually (Frymoyer and Cats-Baril, 1991).
In the last 5 years of the 1990s, Medicare claims demonstrated a 40% increase in spine surgery rates and a 70% increase in fusion surgery rates (Lurie and Weinstein, 2001).
Interestingly enough, the rate of lower back pain is 4 times higher among Swedish, German, and Belgium general populations than among Nigerian, southern Chinese, Indonesian, and Filipino farmers” (Volinn, 1997).
In Sweden 63% of medical secretaries suffer from cervical pain (Kamwendo et al., 1991) while only 32% of office workers in Hong Kong exhibited the same symptoms (Lau et al., 1996).
Such discrepancies are staggering, especially considering the lifestyle of people who live in rural communities compared to industrialized countries.
‘NORMAL’ AND ‘ABNORMAL’ SPINE ARRANGEMENT
We all were educated with firm beliefs of how normal or ideal spines should look. Fig. 1 illustrates a lateral view of a human spine.
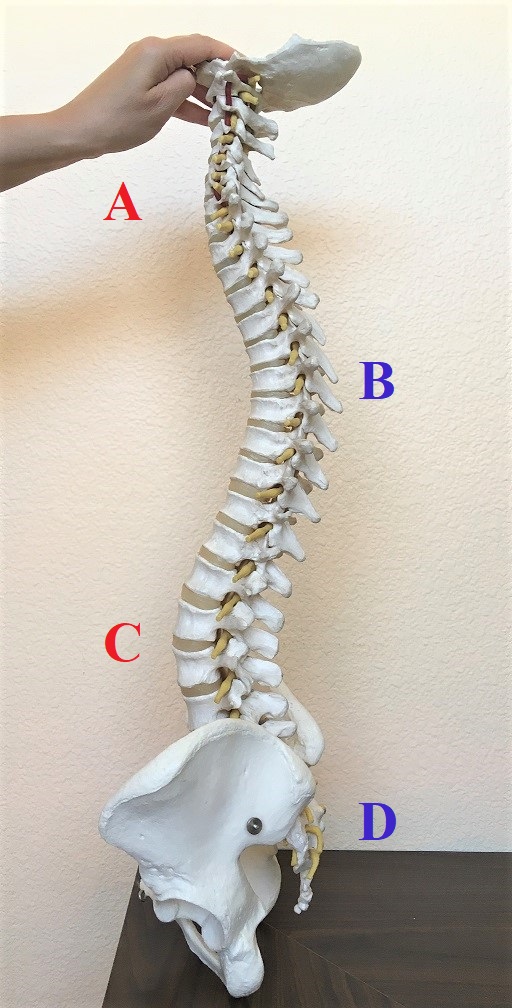
Fig. 1. Lateral view of the ‘normal’ spine
A – cervical lordosis
B – thoracic kyphosis
C – lumbar lordosis
D – sacro-coccygeal kyphosis
While looking at the side view of the spine it is obvious that it exhibits 4 well defined curves which follow each other: cervical lordosis, thoracic kyphosis, lumbar lordosis and sacro-coccygeal kyphosis. Thus, from the side our spine looks like the letter ‘S’ or as a spring which should work as a shock absorber and is supposed to protect our spinal cord from excessive damage during vertically directed traumatic force or age-related wear and tear. If this arrangement is so perfect, why do we suffer so much from disk pathologies which trigger dramatic clinical symptoms?
Everyone knows that disk abnormalities require expensive and complex surgeries with side effects which sometimes leave patients disabled for the rest of their lives. Evolution selected so many great features for us that as a result our bodies became extremely efficient and an effective machine. It is difficult to believe that evolution missed something very important in the anatomical structure of our spine and really failed there. Or didn’t it?
By chance I encountered an interview and writings of Esther Gokhale and some of her ideas stimulated my professional curiosity. She claimed that indigenous people in Africa, Australia, Asia have lower incidents of lower back pain due to the fact that in the difference with Westerns they have lesser spine curvatures. Contrary to S-spine, which we are all familiar with, she called this spine arrangement J-spine (I will continue to use E. Gokhale definition). I decided to examine this issue further since clinical observations in our clinic as well as during last 25 years of practice in the somatic field of the medicine made me come to similar conclusions. Fig. 2 illustrates S-spine and J-spine arrangements.
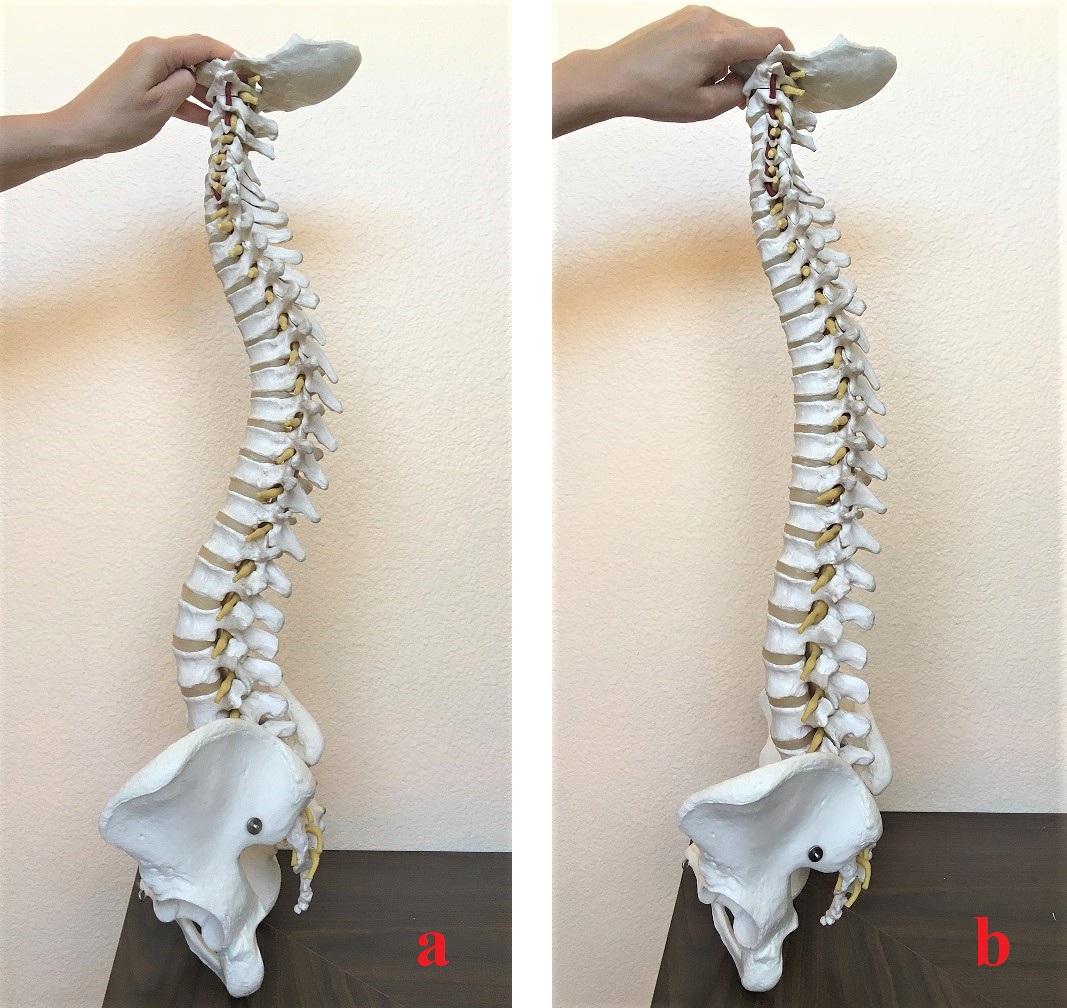
Fig. 2. ‘S’-spine and ‘J’-spine arrangements
a – S-spine arrangement
b – J-spine arrangement
Very frequently we see relatively young patients who came to our clinic with chronic cervical pain and they also exhibited different degrees neurological abnormalities down to the upper extremities. During clinical interview they mentioned that they were diagnosed by having so called ‘military neck’ by a chiropractor or a physical therapist. They were unsuccessfully treated while the neurological symptoms appeared later. Health practitioners who worked on them insisted on the necessity to restore cervical curvature and the patients were advised to sleep with a tightly rolled small towel under the neck since it is supposed to push cervical vertebrae anteriorly while restoring cervical lordosis. From our perspective such practice was the reason for neurological symptoms that appeared down to the arm, forearm and hand adding misery to an already existing cervical pain.
It had always puzzled us why instead of isolating and addressing pain’s initial trigger the practitioners concentrated solely on structural changes making the somatic abnormality more advanced with neurological symptoms joined later. Fig. 3 illustrates an X-ray of the patient after a failed attempt to restore cervical lordosis.
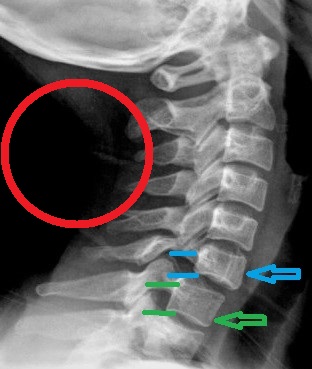
Fig. 3. Anterior Spondylolisthesis of C6 due to unsuccessful treatment of ‘military’ neck
On the X-ray presented in Fig. 3 the patient’s cervical lordosis was indeed restored, but the price was too high. You can clearly see anterior displacement of the entire upper cervical spine from level C6. As a result, the body of C6 was forced to move forward (blue arrow) compared to the body of C7 (green arrow) and its spinal nerve became now squeezed in narrowed neural foramen. Compare the size of neural foramen between C6-C7 (two blue lines) and wider neural foramen between C7-T1 (two green lines).
Despite X-ray success in restoring cervical lordosis, the patient started to suffer from numbness and muscle weakness in the distribution of radial and median nerves. We placed the red circle in the picture to illustrate the position the rolled towel patient is supposed to sleep on during the forced re-creation of cervical curvature. Such treatment indeed displaced upper cervical vertebrae. Similar attempts were made regularly to enlarge lumbar lordosis to a ‘normal’ degree of curvature. It is interesting, but no one actually challenged this notion. How and when was the ‘norm’ we are supposed to follow blindly actually established?
STRUCTURAL ANATOMY OF VERTEBRAL SEGMENT
Fig. 4 illustrates a normal vertebral segment which is formed by two lumbar vertebrae with intervertebral disk in between.
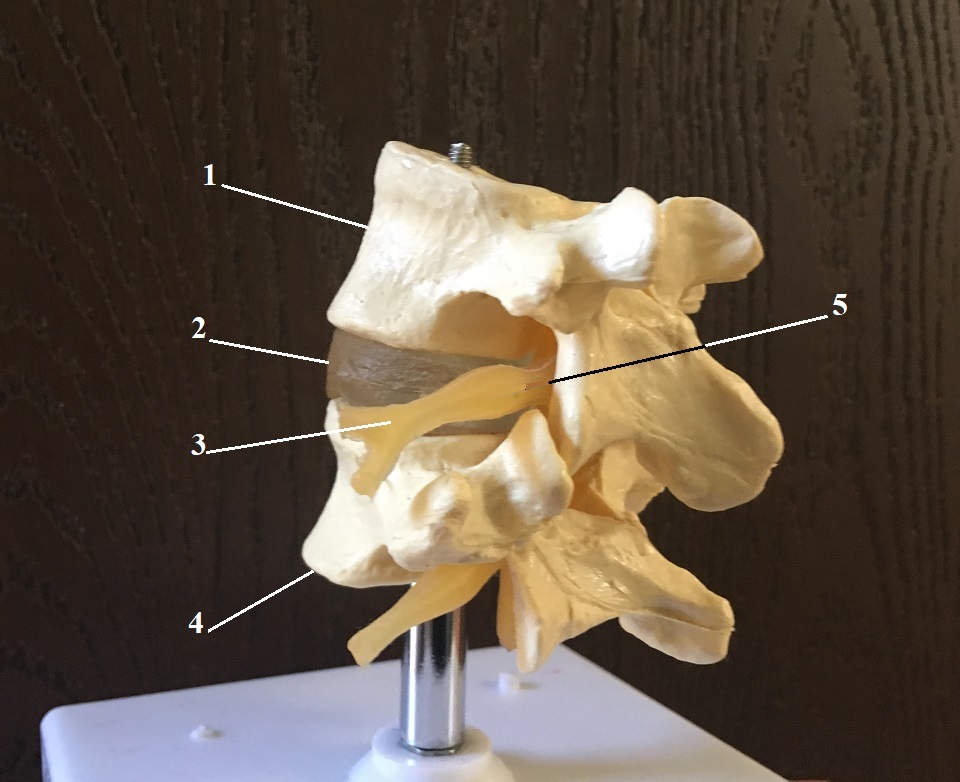
Fig. 4. Lumbar vertebral segment and inner structure of the disk
1 – upper lumbar vertebra
2 – intervertebral disk
3 – spinal nerve
4 – lower lumbar vertebra
5 – neural foramen
Let’s look now at the inner structure of the intervertebral disk. Fig. 5 illustrates the inner structure of the disk.
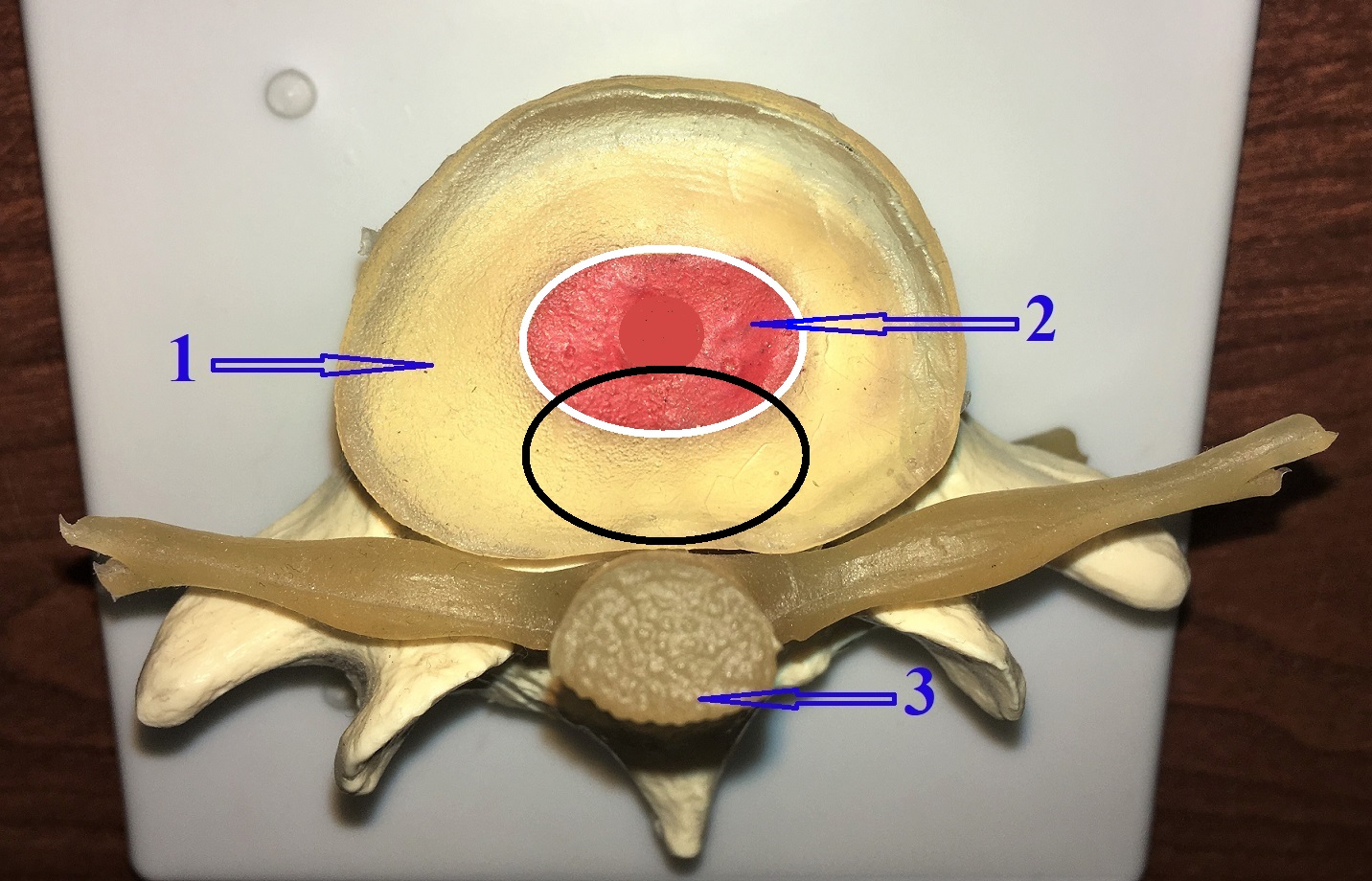
Fig. 5. Inner structure of the disk
1 – annulus fibrosis
2 – nucleus pulposus
3 – spinal cord with spinal nerves
White circle – area for ideal distribution of the vertical load through the disk
Black circle – area of vertical load distribution in cases of excessive S-spine arrangement
A normal disk consists of strong circular cartilage which is called annulus fibrosis and a gel-like inner part called nucleus pulposus. While we are walking, jumping or sitting, the vertical compression of the gel or nucleus pulposus is one of the major contributors to the shock absorbing ability of the spine.
The function of annulus fibrosis is to capture content gel in place allowing it to work as a small shock absorber. Thus, for the disk working properly the vertical load must hit the disk exactly in the middle since that is where the nucleus pulposus is (white circle in Fig. 5).
Surrounding fibers of annulus fibrosis don’t have similar resistance to the vertical compression and as soon as cracks in the annulus fibrosis form, due to its direct traumatization, the inner gel leaks and widens cracks triggering disk pathologies in the form of bulging, herniation and eventually sequestration. Fig. 6 illustrates stages of disk pathology.
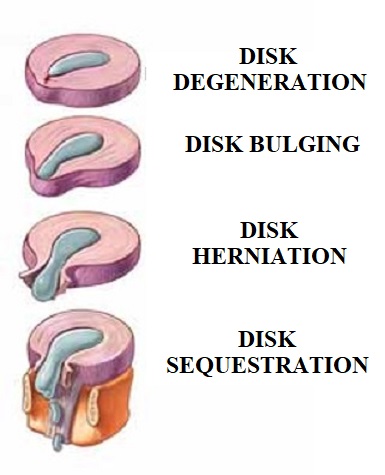
Fig. 6. Stages of disk degeneration
Thus, for the disk to work ideally, the vertical compression must hit the disk in the middle (white circle in Fig. 5) while the S-spine arrangement with excessive curves directs the vertical load to the posterior part of the disk or more precisely, the posterior edge of annulus fibrosus (black circle in Fig. 5). Since fibers of the annulus fibrosis have very limited shock absorbing ability they are not bouncing back and eventually crashed. As a result, the cracks are formed, and it triggers gel leakage and further disk pathologies (see Fig. 6). Thus, if we think logically it is obvious that ‘abnormal’ J-spine arrangement has more health benefits than S-spine arrangement we consider ‘normal’. We will discuss this issue in detail in the Part II of this article.
Meanwhile I encourage readers to look at pictures of world class marathon runners and compare them with regular people. It is obvious that very successful runners have very small curvatures in their spines.
WHY?
Why in Western countries do we have such expressive spine curvatures compared to poor, rural communities in third world countries? Westerners, Africans and Asians all originated from one DNA and have exactly the same body structure and functions, but somehow there are even visual differences in the spine arrangement. Something made our Western spines different due to an unknown factor. Evolution made necessary genetic adjustments to this unknown factor and it may forever have changed the configuration of our spines. This unknown factor must be so commanding that new mutation didn’t wash away over time but instead became dominant and it transferred from generation to generation. These thoughts really occupied my mind for a while until I had a moment of clarity.
Our clinic works with a lot of patients who are team ropers and I was invited to a local rodeo. Sitting and watching ropers compete I realized that the horse was this factor which forever changed the Western spine’s original design of J-spine to our current S-spine configuration.
I would like readers to do some logical thinking before dismissing my ideas completely. While we are walking our legs are close to each other and feet and three major joints work as first shock absorbers before the shock absorbing function of the spine is engaged. A horse rider must spread legs widely and lean forward on the horse. While doing so, the rider increases the pelvis’s anterior tilt. Anterior tilt requires increase of lumbar lordosis and the rider’s body position also increases thoracic kyphosis. To control direction the rider needs to tilt the head backward and that will increase cervical lordosis (see Fig. 7a). Finally, the spread position of lower extremities on stirrups completely disengages the shock absorbing abilities of the feet and significantly decreases it in the three joints of the lower extremities which are now out of the vertical line of load distribution. It forces the shock absorbing abilities of the spine to engage earlier while the rider bounces on the horse and it creates a lot vertical pressure on the spine (see Fig 7b: blue arrow). This pressure must be absorbed somehow before it affects the spinal cord.
Since in the horse rider, shock absorbing abilities of feet and major joints are out of picture, the only way the spinal cord can be protected from the vertical compression which tries to crash the spine is by the increase of shock absorbing abilities of the spine itself. That can be achieved only by increasing the size of cervical and lumbar lordosis and that gives us chronic cervical and lower back pain.

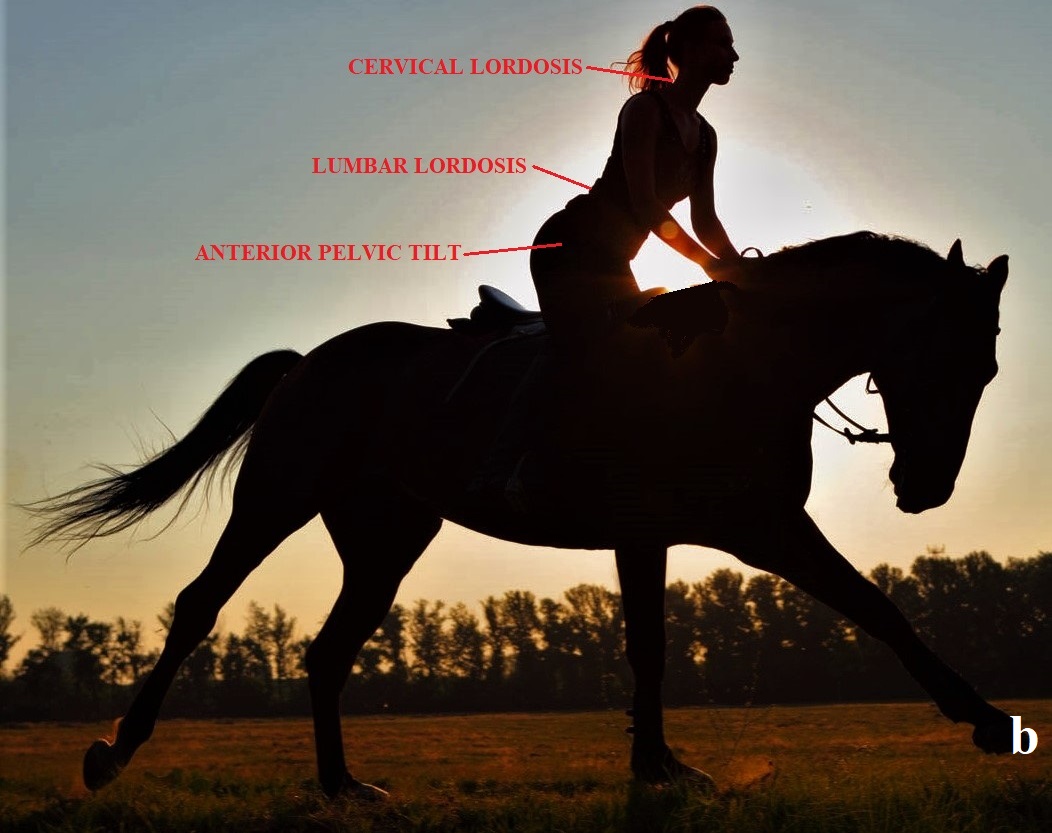
Fig. 7. Vertical impact on the rider (a) and rider’s body position (b) while being on the horse
The population in Africa, Australia and South Asia never used horses so extensively for riding as it was done for millennia in Western and Central Asian cultures. Their spines were never exposed to the bouncing on the horse, sometimes for hours, from a very young age as our Western and Central Asian ancestors did. This is what saved their original J-spine arrangement.
I think readers agree that evolution saves only beneficial mutations in our bodies. This is an optimal tool for our survival. The horse itself was extremely valuable property which increased family wealth, chances for survival, etc. From this basic assumption it is obvious that those of our ancestors who owned a horse(s) had a much better chance of survival and saving their genes compared to those who didn’t own a horse. Thus, while evolution adapted spines of horse riders to new way of vertical load distribution, their DNA had a much better chance to be transferred to future generations. In other words, our so-called ‘normal’ S-spines are our body’s adaptation to the millennia of horse-centered civilizations in Central Asia and in the West.
If my assumption was right our ancestors before horse domestication must have less curvatures in their spines. Thanks to the Internet this assumption can be easily tested and this is exactly what I did. Let’s look at remains of prehistoric people from the times before horse domestication (see Fig. 8).



Fig. 8. Skeletons of prehistoric people
In all these pictures it is obvious that spine curvatures are much smaller and almost abnormal by modern Western standards of ‘norm’ (red arrows). I expect critique that flat spines seen in the pictures are the result of soft tissues decayed with sequential collapse of the bone part of the spine. That not exactly the case since prehistoric people was buried in the ground and not in the coffins and dirt supported their bones while soft tissues were decaying. Also, disks are much firmer, and it takes time for them to decay. These two factors kept bones from pre-historic grave sites close to their original position. If readers pay attention to the Fig. 8‘b’ picture, where one body was placed on the stomach, it is obvious that the spine didn’t collapse since its lumbar curvature and pelvis are clearly visible in elevated position (white arrow).
However, the most striking evidence of low-grade spine curvatures being physiological in our ancestors before horse domestication came from a startling discovery of a practically intact body of Ötzi ice-men.
In September of 1991 a melted ice-sheet in the Alps exposed the body of the hunter who lived 3,400-3,100 years BC. Even the flesh of his body was perfectly mummified by ice and time. This discovery opened our eyes into the pre-historic world, but for our discussion the Ötzi ice-men spine arrangement is an issue of great interest. Fig. 9 illustrates the posterior view of Ötzi ice men.

Fig. 9. Mummy of Ötzi ice-men (3,400-3,100 BC)
As you can see, the pre-historic man had very small spine curvatures (red arrows) and since his soft tissues are still intact it additionally confirms the skeletons’ arrangement in the graves of pre-historic people we discussed above.
There is another aspect in the picture of Ötzi ice-men. As we know the horse was domesticated in the Eurasian steppe approximately 3,500 years BC. Ötzi was contemporary to horse domestication in Central Asia, but more likely he didn’t even see this domesticated animal in Europe since the spread of any new break through was a very slow process and there is a chance that the domestic horse didn’t even get to the pre-historic people who lived in Alps at that time. Thus, his spine wasn’t exposed to the millennia of continuous horseback riding which forever changed our spines to be more adaptive to the horseback-riding S-shape.
In Part II of this article we will discuss scientific data which supports an alternative view on the role of spine curvatures and how and why the issue of S- and J-spine arrangement is so important to therapists who are trying to help patients with chronic cervical and back pain.
REFERENCES
Frymoyer JW, Cats-Baril WL. An overview of the incidences and costs of low back pain. Orthop Clin North Am. 1991 Apr;22(2):263-71.
Kamwendo K, Linton SJ, Moritz U. Neck and shoulder disorders in medical secretaries. Part I. Pain prevalence and risk factors. Scand J Rehabil Med. 1991; 23(3):127-33.
Lau EM, Sham A, Wong KC. The prevalence of and risk factors for neck pain in Hong Kong Chinese. J Public Health Med. 1996 Dec; 18(4):396-9.
Lehrich JR, Katz JM, Sheon RP. “Approach to the diagnosis and evaluation of low back pain in adults”; UpToDate.com; April 2006.
Lurie JD, Weinstein JN. Shared decision making and the orthopedic workforce. Clin Orthop 2001; 385:68-75.
Volinn, E. The epidemiology of low back pain in the rest of the world: A review of surveys in low- and middle-income countries. Spine. 1997;22(15):1747-54.
Category: Medical Massage
Tags: 2019 Issue #2