
Thank you to everyone who shared your expertise in response to our original post. Just as a reminder, the question was what two local conditions can explain the skin reaction to the Compression Test presented in the video.

As correctly mentioned by many therapists, it is true that Thoracic Outlet Syndrome can cause similar reactions on the hand. However, the patient must have numbness and/or burning pain on the entire arm and hand if it is Thoracic Outlet Syndrome (TOS) to blame. If the patient has Anterior Scalene Muscle Syndrome, as a lighter form of TOS, the sensory abnormalities must be present as well, but in lesser form. For example, tingling. The patient didn’t exhibit these symptoms otherwise we would have mentioned them in the original post.
Those of you who mentioned Carpal Tunnel Syndrome were absolutely correct, but it was only one of two pathological scenarios presented in the video. There were a couple of therapists who mentioned Median AND Ulnar Nerve Neuralgias. That is actually the correct answer. The patient exhibits Carpal Tunnel and Guyon’s Canal Syndromes at the same time. The most interesting fact is that the ulnar nerve in the Guyon’s Canal was affected more than the median nerve in Carpal Tunnel.
Please pay attention to the very beginning of the video before testing. The local vasoconstriction, is clearly visible along the hypothenar with the hand hanging in extension under its own weight without a Compression Test even applied. Also, the application of a Compression Test over carpal tunnel triggered more pronounced vasoconstriction on the hypothenar (ulnar nerve distribution) compared to the thenar and the palm (median nerve distribution).
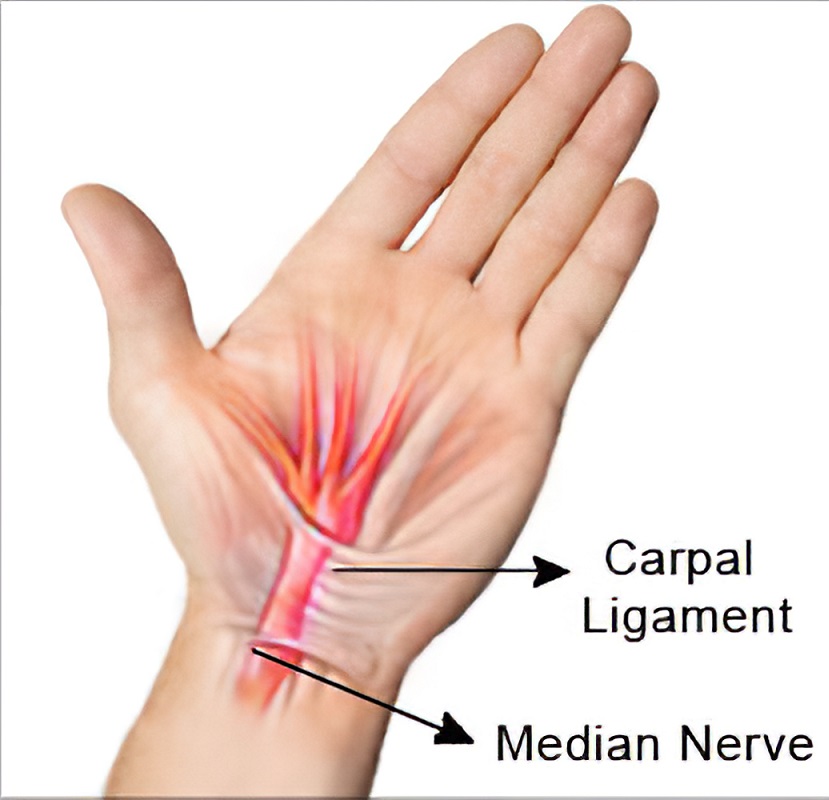
Here is an anatomical situation in the wrist therapists should to consider. The Transverse Carpal Ligament (TLC) forms the roof of the carpal tunnel and lets tendons of flexors with median nerve to pass under it on their way to the palm and fingers. In other words, the carpal tunnel is an entrance gate to the palm. The TCL medially originates from scaphoid and trapezium carpal bones, runs across the palmar wrist and inserts into the hamatum and pisiform bones laterally. Fig. 1 illustrates the position of transverse carpal ligament and its relations with median nerve.
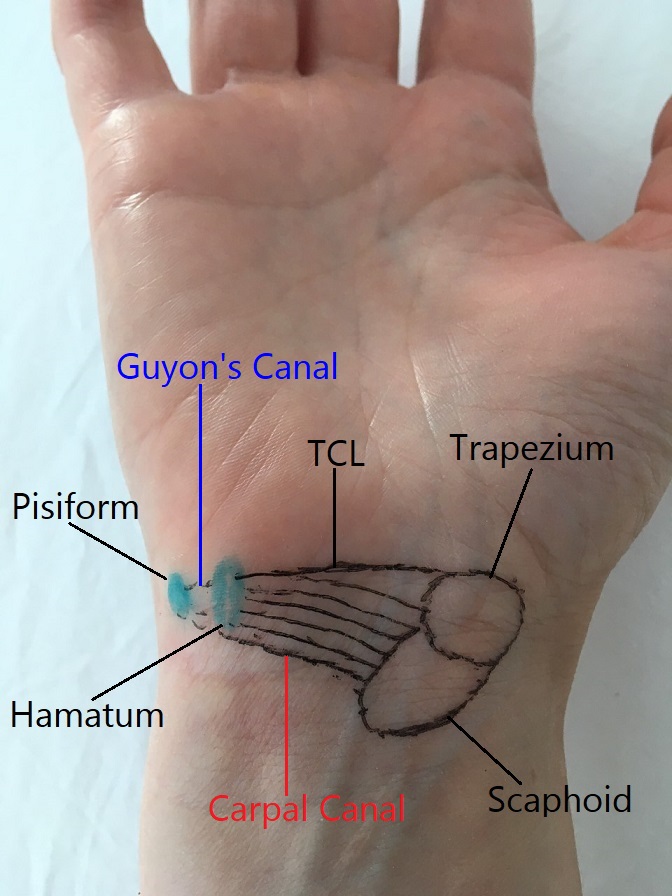
On the ulnar side of the wrist joint medially and more superficially to the TCL is Volar Carpal Ligament (VCL) which originates from the hook of the hamatum bone and inserts into the pisiform bone forming so called Guyon’s Canal. Thus, walls of this very narrow and short, but clinically important canal, forms medially by the hook of hamatum, laterally by pisiform bone, on the bottom by TCL and roof of it is VCL. Fig. 2 illustrates the anatomy of Guyon’s Canal.
Guyon’s canal contains ulnar nerve and artery. Technically speaking some fibers of TCL are contributing to more superficially positioned VCL. Thus, tension and scarification of TCL may also affect VCL and vice versa. In such cases therapists are going to observe a mixed clinical picture of Median and Ulnar Nerve Neuralgias at the same time.
The Compression Test presented in the video additionally stressed TCL to examine the degree of pressure formed in the carpal canal. The test indeed indicated the median nerve entrapment within carpal canal since the new sensations on the palm were reported by the patient and visual signs of vasoconstriction appeared on the thenar (they are clearly visible in the video). However, vasoconstriction was much more prominent on the hypothenar which is ulnar nerve distribution.
Thus, we are dealing with Median Nerve Neuralgia and Ulnar Nerve Neuralgia at the same time with ulnar nerve more compressed within Guyon’s Canal than median nerve within Carpal Canal.
It is obvious that these changes are work related. Repetitive motions and the pressure generated during massage strokes are initial triggers. Many therapists are using the pisiform bone as an additional pressure tool during the deep strokes. Another aspect is scarification of TCL which secondarily decreases the cross section of Guyon’s Canal due to the medial displacement of the pisiform bone and it compresses the ulnar nerve first since this canal is very narrow compared to the carpal canal.
Let’s look at both canals in close proximity. Fig. 3 Illustrates relations between Carpal and Guyon’s Canals.
From the treatment perspective both canals must be decompressed separately with Guyon’s canal as a priority in this clinical case. Since Guyon’s canal is very narrow the therapist is forced to work with precision at the insertions of VCL to the hamatum and pisiform bones, decrease adhesions between skin with subcutaneous tissues and VCL and finally stretch Guyon’s Canal itself, separately from the Carpal Canal which should be worked in the second part of the session. Remember that in the difference with Carpal Canal, Guyon’s Canal is superficial and shallow with both ulnar nerve and artery on the bottom of it against carpal bones. Be very careful with the degree of applied pressure. While working in the canal and on its walls ask the patient to report any new sensations on the hypothenar, pinky and half of the 4th finger. If sensations appear, immediately decrease the amount of applied pressure.
Fig. 4 Illustrates position of the finger to work on medial wall of Guyon’s Canal (hook of hamatum).

Fig. 4. Finger position to address insertions of VCL to hook of hamatum bone
Arrow is direction of pressure
Fig. 5. Illustrates position of the finger to work on lateral wall of Guyon’s Canal (pisiform bone).

Fig. 5. Finger position to address insertions of VCL to pisiform bone
Arrow is direction of pressure
Finally, Fig. 6 illustrates manual decompression of the Guyon’s Canal in in perpendicular directions and Fig. 7 in longitudinal direction. Please note that stretch along the canal requires combination of forces: stabilization of the hamatum bone with one finer, the wrist extension with simultaneous radial deviation.

Fig. 6. Stretching of Guyon’s Canal in perpendicular direction
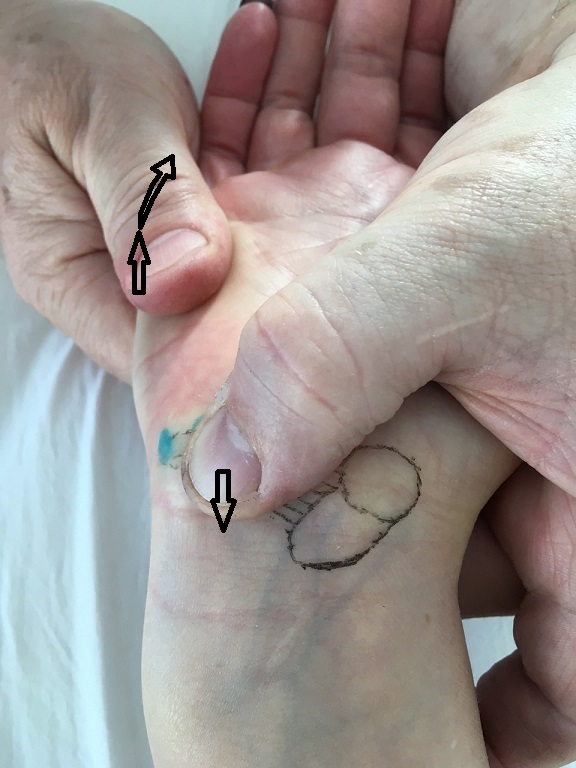
Fig. 7. Stretching of Guyon’s Canal in longitudinal direction
Category: Blog