
By Dr. E. Gubsky (Republic of Belarus)
Oleg Bouimer, LMT, CMMP (Los Angeles, USA)
From the outset, we would like to state that vibration is not just a ‘feel good’ application but an essential tool in significantly increasing the clinical effectiveness of Massage Therapy.
In addition to developing a skill for manual vibration, therapists should also have some electric vibration devices in the professional toolbox. Let us take a closer look at the science behind vibration and its effects on the human body.
General Overview
Vibration is a potent stimulus for all living organisms. It surrounds us in everyday life and is produced by different inner and outer sources. The human body itself is a complex vibro-mechanical system. Every internal organ and system is affected by vibration during each body movement. The beating of the heart and pulsation of the large vessels are constant sources of inner vibration. Any external source of vibration also evokes a variety of physiological responses.
The vibration was considered an essential therapeutic tool since the dawn of medicine. The Roman physician Galen, who lived in the second century AD, was the first to incorporate a vibration technique in massage therapy.
At the beginning of our century, vibration massage (VM), especially electric vibration, was one of the most frequently used physiotherapy methods. Professor A. Sherbak, MD (1903) in Russia, and Dr. M. Snow, MD (1917) in the USA were pioneers in examining the effects of electric vibration on the human body in experimental and clinical studies.
In the USA, after World War II, VM was forced out by other physiotherapy methods. In recent years, the clinical effects of vibration re-gained the interest of the medical community. However modern medicine continued to accumulate a large body of scientific data on the clinical benefits of electric vibration and usage of a Whole-Body Vibration Platform, Massage Chairs, and different handheld electric massagers. Let’s review this data.
Vibration And Its Effect On The Human Body
The human body is made up of 50-60% water. Such a high-water content allows vibratory stimuli to travel far from the area of initial application, the same way that waves ripple after a stone is thrown into a lake.
Suppose a practitioner applies vibratory stimuli in the correct place and at the correct angle to the body’s surface. In such a case, they may directly stimulate or inhibit functions of the somatic or visceral structures affected by trauma or a pathological process.
The primary receptors which analyze and encode the vibration are called Pacinian Corpuscles (PC). They are in the skin’s dermis, in the subcutaneous tissue, in the bones’ periosteum, and many inner organs (pancreas, intestinal walls, breast, sex organs, etc.).
PCs are not spread equally throughout the body. Therefore, we feel a vibration in different parts of the body to various degrees. The structure of the Pacinian corpuscle is shown in Fig. 1.
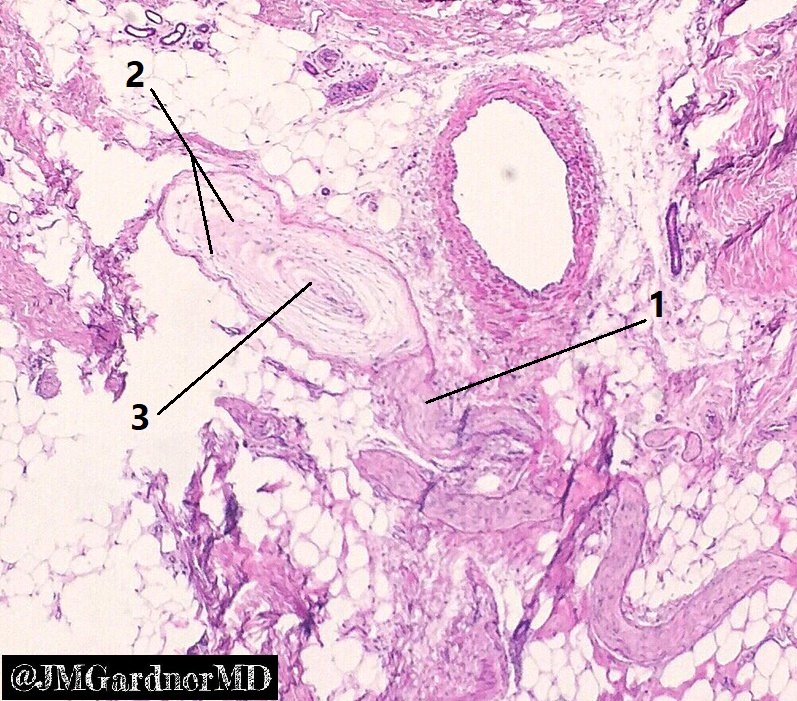
1 – branch of peripheral nerve
2 – receptor’s capsule
3 – nerve ending
PC is an approximately 1mm long oval-shaped receptor. The entire corpuscle consists of the nerve ending projecting into the middle of the receptor and the capsule, which surrounds the nerve ending, composed of 20 to 60 concentric layers of connective tissue separated by gelatinous material which consists of 92% water.
PC works in two ways:
- PC as a pressure receptor. When the therapist compresses and steadily maintains pressure, he or she deforms the capsule and nerve ending. When a nerve ending gets deformed, it fires sensory data to the brain, and we feel a sense of soft tissue compression.
- PC as vibration receptor. When a therapist uses manual or electric vibration, he or she alternates the application and release of compression stimuli. Every compression/release fluctuation deforms the capsule’s gelatinous material, and as a result, the nerve ending fires separately for the compression stage and pressure release stage (Loewenstein and Skalak, 1966). When these compression/release alternations reach the brain, it forms a sense of vibration we feel.
PCs can detect vibration in the range between 50 and 6000 Hz. From a treatment perspective, 50-120 Hz frequency is the optimal treatment regime. Only electric vibration may produce such frequency.
It’s important to remember that PCs are rapidly-adapting receptors (Macefield, 2005). The degree of a receptor’s adaptation is how quickly it stops to fire up to the CNS during continuous exposure to the same stimulation.
To continually keep PCs firing and stimulate CNS, vibratory stimuli have to be removed and immediately reapplied. On the contrary, to stop PCs from firing while simultaneously inhibiting the CNS, the therapist should continue to apply the vibration in the same place without changing position or moving the device along the segment.
In addition to PCs, vibration activates deep receptors located in the ligaments, tendons, and periosteum. However, these receptors are firing later after the vibration was already applied to the same area. Their activation is a secondary result of the effect of vibratory stimuli on circulation.
Clinical Effects Of Vibration
Vibration has many therapeutic effects on the human body. Based on the analysis of experimental and clinical publications, VM has the following clinical effects:
Analgesic Effect
The flow of ascending or afferent stimuli from PCs reaches the posterior horns of the spinal cord. From there vibration stimuli, along with nociception (i.e., pain perception) and temperature sensibility, reach the sensory cortex located in the temporal lobes. Since nociception and vibration travel together to the same brain areas, vibration to the affected area with a frequency around 100Hz has a potent analgesic effect (Kreymer, 1986).
Vibratory stimuli can block any other sensory stimuli (pain, itch, tension, etc.) to the degree of complete desensitization of all peripheral receptors in the treatment area. The complete inhibition of the sensory centers in the CNS achieved if vibration introduced to the tissues before any irritating or pain-generating stimuli (Hagbarth and Eklund, 1966).
Additionally, vibration has a positive effect on the nociceptors’ (a.k.a. pain perception) activity by restoring their activation threshold. If the patient has trauma or inflammation, the normal threshold of nociceptors’ activation drops. In such cases, even mild touch starts to trigger acute pain, while in normal areas, the same intensity of touch does not cause any discomfort. Thus, when applied to the nociceptors in the affected area, the mechanical energy generated by vibration restores their physiological threshold and blocks pain perception (Razumov, 1975).
Electric vibration has a profound impact on all peripheral receptors in the stimulated area. When the contact area of the massager touches the soft tissues, touch, pressure, vibration, noci- and later temperature receptors fire simultaneously to the segment(s) of the spinal cord responsible for the innervation of the area the therapist works on. However, the vibratory stimuli remain the most powerful and they override pain perception (Kreymer, 1987; Gilman, 2002).
The unique clinical effect of vibratory stimuli on the CNS was examined and explained in detail by the fathers of the Gate-control Theory of Pain, Prof. R. Mezlack and Prof. P. Wall (1965). According to the authors, at the first moment of exposure of the tested area to vibration stimuli, they stimulate high-intensity pain and itch. Still, later on, pain and itch are inhibited. Thus, “…the overall effect of permanent vibration is strong pain inhibition” (Mezlack and Schecter, 1965).
Therefore, electric vibration is a vital component of any Trigger Point Therapy session. The efficient desensitization of the peripheral receptors before application of ischemic compression greatly assists in the complete and stable elimination of active trigger points.
Recently Bidonde et al. (2017) registered significant improvement in the clinical picture of Fibromyalgia patients after a course of whole-body vibration therapy due to the same effect of peripheral desensitization.
Vasomotor Effect
The immediate effect of vibration applied to the stimulated area is vasospasm. However, after prolonged application (up to one minute), the circulatory system reacts with potent vasodilation. Thus, vibratory stimuli have a powerful vasomotor effect (Chizik et al., 1983; Skoglund, 1999).
Another unique clinical feature of vibration is its distant vasomotor reflex. For example, the application of permanent vibration on the lower back area, according to Glezer/Dalicho Zones (1955), of patients with obstructive arterial disorders produces peripheral vasodilation and an increase of arterial circulation in the legs and feet. It is registered as an average increase of the feet’ temperature up to 0.94 C (Kreymer, 1987).
A study conducted by Zange et al. (2014) indicated that electric vibration activates venous drainage by ejecting capillary, venous blood from muscle tissue. Venous blood drainage helps muscle recovery from tension triggered by chronic overloads, and it also speeds up tissue rehabilitation after acute muscle spasms.
A fascinating study conducted by Rodriguez-Miguelez, et al., (2015) concluded that electric vibration’s application maintains blood’s fluidity and significantly decreases the concentration of inflammatory substances (cytokines and interleukins), eliciting long local anti-inflammatory effects.
Effect On The Musculoskeletal System
High-frequency interruptive vibration activates the motor centers in the spinal cord, stimulating the skeletal muscles. This effect of interruptive vibration is beneficial in muscle atrophy, Flaccid Palsy after a Stroke, etc. (Ivanenkova, 1968). On the contrary, low-frequency fixed vibration inhibits motor centers and decreases muscle tone (Bierman, 1960).
Electric vibration is a beneficial therapy for patients with Parkinson’s Disease since it removes desynchronization of the movements in Parkinson’s patients and places their motor cortex in a more ‘ready‐to‐move’ state (Marcello et al., 2018).
An experimental study on animals indicated that the application of high-frequency electric vibration elicits muscle tonic contractions. Hagbarth and Eklund, (1966) called this phenomenon Tonic Vibration Reflex (TVR). TVR originates in the muscle spindle receptors as soon as the muscle is exposed to the vibration. As soon as the sensory input from muscle spindle receptors reaches the spinal cord, the lower motor centers send descending commands to the same muscle, triggering its tonic contractions (Johnston et al., 1970; Zaidell, et al., 2013).
This effect of TVR is essential for patients with muscle weakness since it increases the tonic contractions of the muscles affected by muscle atrophy, flaccid palsy after stroke, etc. (Myamoto et al., 1967). Simultaneously, TVR decreases the muscles’ spasticity affected by Parkinson’s Disease (Macerollo et al., 2018). Initially, the spasticity increases after vibration application, but it drops below the original level with the prolonged application.
The practitioner may facilitate the intensity of TVR by asking the patient to slightly increase voluntary tension in the muscles exposed to permanent vibration, or what is even more interesting, to moderately contract the muscles on the opposite, untreated side (Johnston et al., 1970, Tochigi et al., 1977). That is clear evidence that the CNS plays a regulatory role in the generation and maintenance of TVR.
Thus, TVR has a unique dual clinical effect: it increases tonus and contractile ability of the weak muscles and decreases elevated muscle tone of spastic muscles. One can say that TVR helps to readjust pathologically changed muscle tone. The positive effect of whole-body vibration on skeletal muscle mass and bone density are well-established facts (Davis et al., 2010; Chen et al., 2017; Bemden et al., 2018).
Effect On The Endocrine System
The application of VM stimulates the function of the adrenal and pituitary glands (Piechocinski,1986). At the same time, the thyroid gland shows signs of hypofunction (Kreymer, 1987).
Whole-body vibration makes soft tissue more sensitive to insulin, and it can be used as an additional tool to control Diabetes (McGee-Lawrence, et al., 2017.)
This concludes Part I of the article. Thank you for taking the time to read through it! Hopefully, it has provided you with enough information to see the value of adding this clinical tool of massage therapy to your toolbox. In Part II of this article, we will discuss the vibration treatment regime therapists should use in different clinical cases.
REFERENCES
Bemben D., Stark C., Taiar R., Bernardo-Filho M. Relevance of Whole-Body Vibration Exercises on Muscle Strength/Power and Bone of Elderly Individuals. Dose-Response. 2018 Oct-Dec; 16(4): 1559325818813066.
Bidonde J., Busch A.J., van der Spuy I., Tupper. S., Kim S.Y., Boden C. Whole body vibration exercise training for fibromyalgia. Cochrane Database Syst Rev. 2017 Sep; 2017(9): CD011755.
Chen H., Ma X., Lu B., Ma X. The effect of whole-body vibration training on lean mass A PRISMA-compliant meta-analysis. Medicine (Baltimore). 2017 Nov; 96(45): e8390.
Chizik, V.I., Trapaznikova, N.K., Bistrova, I.I., Mihailova, E.V. The Effect of Vibromassage on the Rehabilitation of the Lower Extremity after Trauma of the Sciatic Nerve. VIII Congress of Physiotherapists, “Medicina”, Moscow, 133-134, 1983.
Davis R., Sanborn C., Nichols D., Bazett-Jones D.M, Dugan E.L. The effects of whole-body vibration on bone mineral density for a person with a spinal cord injury: a case study. 2012 Dec. 4(12):963-75.
Gilman S. Joint position sense and vibration sense: anatomical organization and assessment. J Neurol Neurosurg Psychiatry 2002;73:473–477
Glezer, O., Dalicho, V.A. Segmentmassage. Leipzig, 1955.
Hagbarth K.E., Eklund, G. "Tonic Vibration Reflexes (TVR) in Spasticity." Brain Res., 2: 201-203, 1966.
Johnston, R.M., Bishop, B., Coffey, G.H. Mechanical Vibration of Skeletal Muscles. Phys. Ther., 50:4, 499-505, 1970.
Ivanenkova, E.D. Vibration Massage in Cases of Trauma and Disorders of the Muscle-Skeletal System. Vopr. Kurortol. Fizioter. Lech. Fiz. Cult. 33(6): 525-528, 1968.
Kreymer, A.Y. Vibration Massage at Diseases of the Nervous System. Tomsk University, Tomsk, 1987.
Loewenstein W.R, Skalak, R. Mechanical transmission in a Pacinian corpuscle. An analysis and a theory. J Physiol. 1966 Jan; 182(2): 346–378.
Macefield V.G. Physiological characteristics of low-threshold mechanoreceptors in joints, muscle and skin in human subjects. Clin Exp Pharmacol Physiol, Jan-Feb 2005;32(1-2):135-44.
Macerollo A., Palmer C., Foltynie T., Korlipara P., Limousin P., Edwards M., Kilner J.M. High‐frequency peripheral vibration decreases completion time on a number of motor tasks. Eur J Neurosci. 2018 Jul; 48(2): 1789–1802.
McGee-Lawrence M.E., Wenger K.H., Misra S., Davis C.L., Pollock N.K., Elsalanty M., Ding K., Isles C.M., Hamrick M.W., Erion J.R., Wosiski-Kuhn M., Arounleut P., Mattson M.P., Cutler R.G., Yu, J.C., Stranahan A.M. Whole-body Vibration Mimics the Metabolic Effects of Exercise in Male Leptin Receptor Deficient Mice. Endocrinology, 2017 DOI: 10.1210/en.2016-1250
Mezlack, R., Schecter, B. Itch and Vibration. Science, 147(Feb): 1047-1048, 1965.
Mezlack, R., Wall, P. Pain Mechanism: A New Theory. Science, 150 (Nov): 971-979, 1965.
Myamoto, S., Okamoto, M, Hori, G. Clinical Application of Tonic Vibration Reflex Stimuli and Tonic Vibration Reflex." in Proc. Int. Symp. Tonia Vibr. Reflex, p. 121-137, Kyoto, 1967.
Piechocinski, R. Effect of vibration on the morphologic pattern of endocrine glands. Pat Pol., 17(4): 561-563, 1986.
Razumov, I.K. Theoretical Foundations of the Effects of the Vibration on the Human Body. Medicine, Moscow, 1975.
Rodriguez-Miguelez P., Fernandez-Gonzalo R., Collado P.S., Almar M., Martinez-Florez S., de Paz J.A., González-Gallego J., Cuevas M.J. Whole-body vibration improves the anti-inflammatory status in elderly subjects through toll-like receptor 2 and 4 signaling pathways. Mech Ageing Dev. 2015 Sep; 150:12-9.
Sherbak, A.E. Further Experimental Studies of the Physiological Effects of Mechanical Oscillations. Psych. Review, 9: 641-649 and 10: 722-733, 1903.
Skoglund C.R. Vasodilatation in human skin induced by low-amplitude high-frequency vibration. Clin Physiol, 1999 Aug;9(4):361-72.
Snow M.L. Mechanical Vibration. Its Physiological Application in Therapeutics. New York, 1917.
Tochigi, S., Nakano, Y, Kawaguchi, S., Wanatabe, S. Clinical Assessment of Tonic Vibration Reflex. Vibratory Stimuli and the Tonic Vibration Reflex; in Proc International Symposium Tonic Vibration. Reflex, Tokyo, 151-152, 1977.
Zaidell LN, Mileva KN, Sumners DP, Bowtell JL. Experimental evidence of the tonic vibration reflex during whole-body vibration of the loaded and unloaded leg. PLoS One. 2013 Dec 30;8(12):e85247.
Zange J., Molitor S., Illbruck A., Müller K., Schönau E., Kohl-Bareis M., Rittweger J. In the unloaded lower leg, vibration extrudes venous blood out of the calf muscles, probably by direct acceleration and without arterial vasodilation. Eur J Appl Physiol. 2014; 114(5): 1005–1012.

Dr. Evgeny Gubsky graduated from the Belorussian State Medical University. He has been a general medicine and massage therapy practitioner for over ten years. Dr. Gubsky is an active blogger and educator specializing in the rehabilitation of injured athletes using massage therapy and other clinical tools. He is the creator of the Massage Solutions website, which gives therapists all tools required to incorporate electric vibration into their practice:
https://massagesolutions.net/

Oleg Bouimer, LMT, graduated from State Institute of Physical Education in Ukraine in 1985. Currently he has an extensive private practice in Los Angeles. Among his clients are celebrities, famous politicians and sports stars. The NBA, NHL and NFL widely recognize Oleg and the system of Russian Sports Massage. He teaches nationwide and has founded a Medical and Sports Massage Club in Los Angeles. Oleg is author of many articles in American and European professional journals. His main educational website: www.russiansportsmassage.com
Category: Medical Massage
Tags: 2021 Issue #1
