
Original Question:
This post is intended for therapists who practice the clinical aspects of Massage Therapy. A patient came to our clinic with an acute left lower back pain history. He was treated in pain and PT centers for several months without achieving stable results.
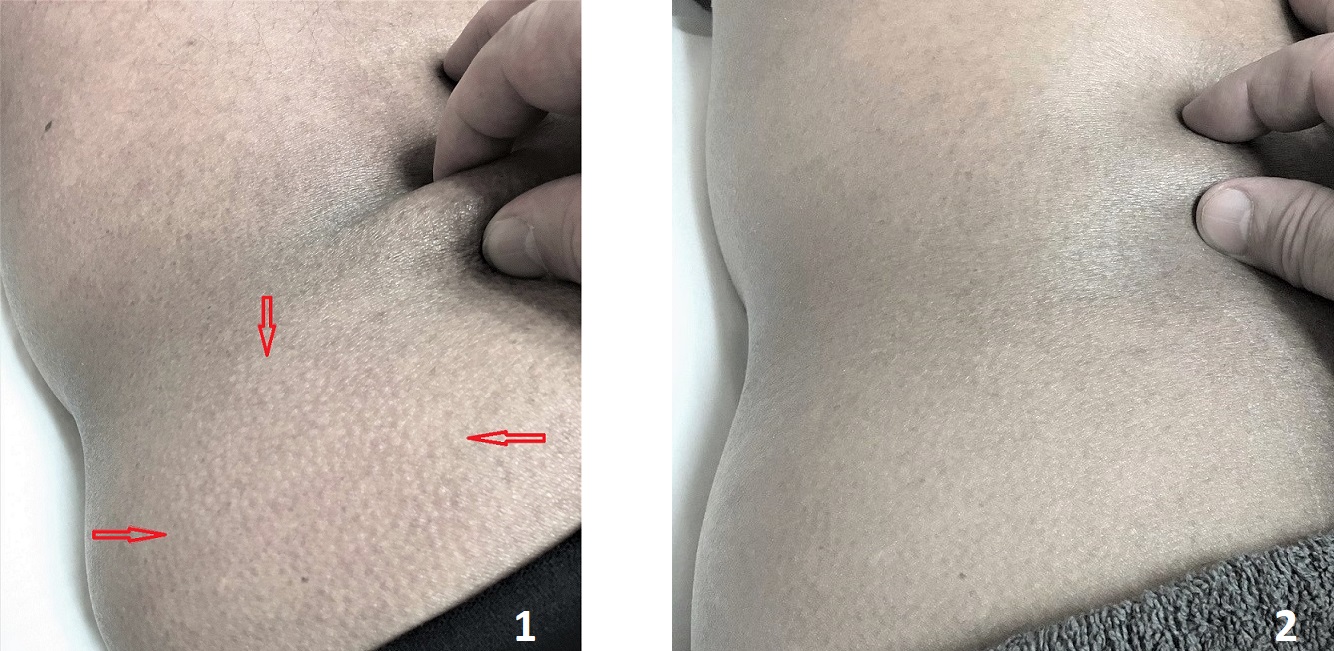
Picture 1 illustrates the application of the second part of Dr. Kibler’s Technique in his left lower back to examine the degree of tension in his superficial fascia. Every time we tried to lift a fold of skin on the patient’s lower back, goosebumps appeared on the skin in his left gluteal area (red arrows), the intensity of lower back pain sharply increased, and he felt warm wave spread down his left lower extremity. As soon as the skinfold was released (picture 2), the goosebumps diminished or went away entirely while the warm wave stopped. When we reapplied Dr. Kibler’s Technique, everything returned.
How should a therapist interpret this clinical sign?
Thank you to everyone who posted their answers! The patient’s body during evaluation and treatment delivers priceless data in the form of constantly changing clinical signs and symptoms. The ability of the therapist to read and correctly interpret them is the foundation of clinically successful Medical Massage practice. That is why SOMI invests so much time and effort in educating our students in these vital professional skills.
ANSWER:
Those therapists who mentioned fascial tension were correct. However, the events shown in the pictures have more complexity than just fascial tension.
The second part of Dr. Kibler’s Technique examines the degree of reflex tension formed in the superficial fascia called active Connective Tissue Zones (CTZs). By lifting the fold of skin in the area of active CTZs and comparing results with unaffected areas, a therapist can detect the degree of adhesions formed between the skin with subcutaneous tissue and superficial fascia, which covers superficial skeletal muscles. More restrictions to the skin lifting, more adhesions between layers, and more tension formed in the superficial fascia.
The CTZs may form as a response of fascia to incorrect innervation, trauma, or visceral disorders (for example, pulmonary disorders, kidney dysfunction, etc.). To a different degree, CTZs is always present in patients with chronic pain.
The correct execution and interpretation of Kibler’s Technique give the therapist the necessary information about the degree of tension in the superficial fascia. However, the formation of ‘goose bumps’ during the examination of fascial tension illustrates an entirely different phenomenon.
Active CTZs are strongly associated with an autonomic nervous system, which controls all our body functions. Thus, goosebumps shown in the original picture are a sign of profound disbalance within sympathetic and parasympathetic divisions of the autonomic nervous system rather than a degree of fascial tension.
When active CTZs are aggressively examined or treated (which is frequently the case), they may trigger autonomic reactions seeing as local sweating, goose bumps, nausea, headache, increased or respiratory (tachypnea) and heart rate (tachycardia), etc. When autonomic reactions are triggered, the patient may experience discomfort for hours and even days following the treatment session and will never return to that same therapist. In other words, aggressive treatment in active CTZs also widens the gap between sympathetic and parasympathetic divisions of the autonomic nervous systems. That is why patients may feel unwell after an incorrectly chosen treatment strategy.
To avoid autonomic reactions, the therapist should ask the patient beforehand to immediately inform them of any new changes or sensations they start to feel. The therapist should continuously observe tissue reactions to the examination and/or treatment. Local sweating exhibited by the patient is one of the first signs that the therapist is on the edge of triggering an autonomic reaction.
As soon as this clinical sign appears, the therapist must immediately decrease the intensity of the treatment and switch to a different set of techniques (e.g., inhibitory regime) or another part of the body. If autonomic reactions are fully triggered, sometimes even after the end of the session, there is no way to stop them. Of course, these reactions will disappear in several hours or days. Still, the patient feels unwell throughout, while the autonomic reactions further reinforce the imbalance of the autonomic nervous system.
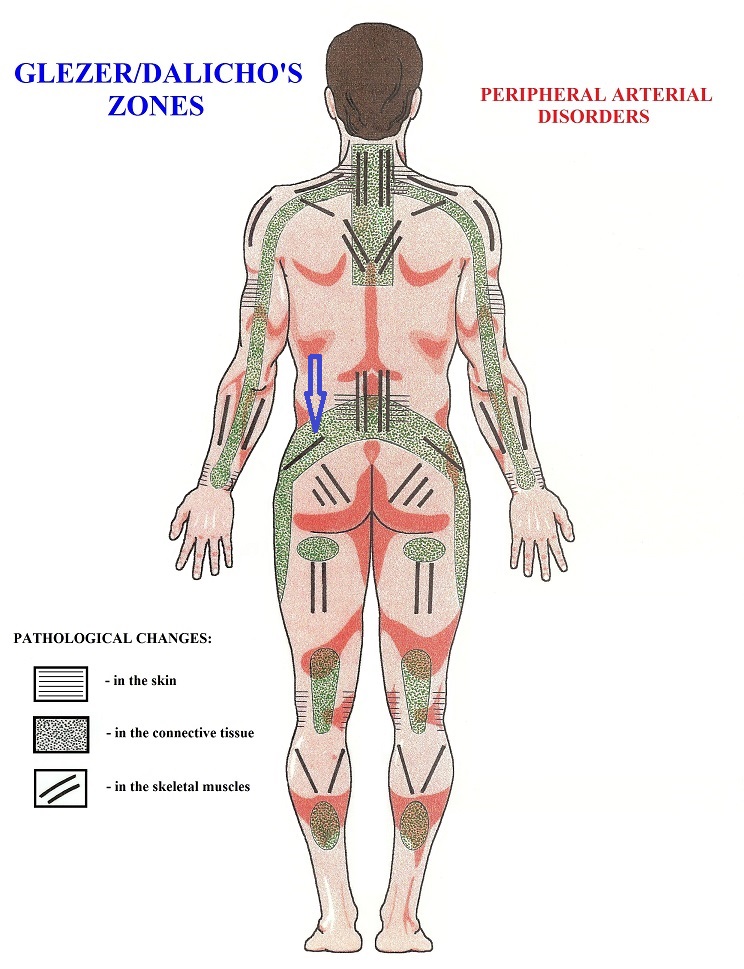
The final piece of the puzzle. Why did the patient feel warm sensations along the left lower extremity during the execution of Kibler’s Technique? The answer to this question is in the unmatching clinical value of Dr. Glezer/Dr. Dalicho maps of reflex zones. Please examine the Figure below, which presents the distribution of reflex zones in the soft tissues in cases of vascular abnormalities. The fascial tension (green dotted area emphasized by the blue arrow) spreads distally from the lower back along the lateral thighs, and it may trigger local vasoconstriction downward.
The CTZs are very responsive to the therapy when it is done correctly. In this case, even a simple examination while the skin is lifted slightly decreases the tension in the superficial fascia. In turn, it temporarily diminishes activity within CTZs by stretching the adhesions formed between tissue layers. Finally, via the reflex vasculatory mechanism, these events trigger reflex vasodilation, which the patient feels as warm waves moving down to the lower extremity.
Thus, a ‘domino effect’ links pathological changes in the human body in one logical chain of events. By knowing and understanding the rules of the ‘domino effect’, the therapist can may dramatic improvements in the health of patients and build a successful practice.
Many therapists expressed interest in learning more about Dr. Kibler’s Technique which consists of two parts. The first part examines the tension in CTZs located in the skin’s dermis, while the second part examines CTZs formed in the superficial fascia. Third-level of CTZ is located in the deep fascia, and the therapists should use the Opposite Shift Technique to rule in or rule out tension formed in the deep fascia, which separates superficial and deep muscle groups.
To learn more about this and other critical evaluation and treatment techniques of Massage Therapy, join SOMI’s Live Seminars and Webinar. The information and data we share with therapists are of unprecedented importance, and you do not find it in any other educational sources. We built the bridge between medicine and massage therapy using only scientific and clinical data. Please visit Medical Massage Courses & Certification | Science of Massage Institute for details.
Category: Blog