
ORIGINAL QUESTION
A patient presented to our clinic with severe posterior neck and upper-shoulder pain, headache, and “pins and needles” sensations along the radial side of the forearm extending to the left thumb. The elevation of the left shoulder and protrusion of the left clavicle are clearly visible. The patient is right-handed. Cervical ROM was moderately restricted.

Question: What is the likely trigger for these symptoms based on visual assessment?
ANSWER TO CHECK YOUR CLINICAL REASONING #10
by Dr. Ross Turchaninov
Thank you to everyone who posted comments under the original post. Let us summarize the suggested triggers:
- Cervical radiculopathy
- Traumatic injury
- Poor ergonomics
- Cervical muscle spasm
- Scoliosis
- Tension in the pectoral muscles
- Rib subluxation
- Tension in the supraspinatus muscle
- Tension in the levator scapulae muscle
- Tension in the subscapularis muscle
- Tension in the trapezius muscle
- Tension in the semispinalis muscle
- Abnormalities in the lower extremity and pelvis
- Fascial torsion
- Diaphragmal spasm
Those who identified Anterior Scalene Muscle Syndrome (ASMS) were absolutely correct (the explanation follows below). Several therapists mentioned Thoracic Outlet Syndrome (TOS). Although both conditions share a similar mechanism, they differ clinically.
Patients with classic TOS typically present with irritation of more than one peripheral nerve, and the intensity of peripheral neuropathic symptoms is severe. Anatomically speaking, the ‘thoracic outlet’ is a small triangular space above the clavicle between the tendinous parts of the anterior and middle scalene muscles. This space is for the subclavian artery to pass through, with the subclavian vein anterior to it. Thus, all patients with TOS must demonstrate some circulatory involvement, such as delayed venous drainage due to subclavian vein compression or peripheral vasoconstriction caused by subclavian artery compression.
Finally, two therapists correctly mentioned possible entrapment of the accessory nerve (cranial nerve XI)—Bravo!
Let us now examine this clinical case in greater detail.
The spasm of the left trapezius muscle is the first visible clue and can provoke posterior neck and shoulder pain, as well as occipital headaches, by increasing pressure in the suboccipital space. However, it is highly unlikely that trapezius muscle spasm alone would irritate the radial nerve and produce symptoms radiating down the left forearm and into the thumb.
For trapezius spasm to be forceful enough to irritate the radial nerve, it would need to restrict all rotations between cervical vertebrae completely. In such a scenario, the patient would be unable to rotate the head. However, our patient retained the ability to rotate the head, though with moderately reduced ROM. This raises a critical question:
Does trapezius spasm cause the patient’s symptoms, or are both the symptoms he has and the trapezius spasm secondary to another underlying trigger?
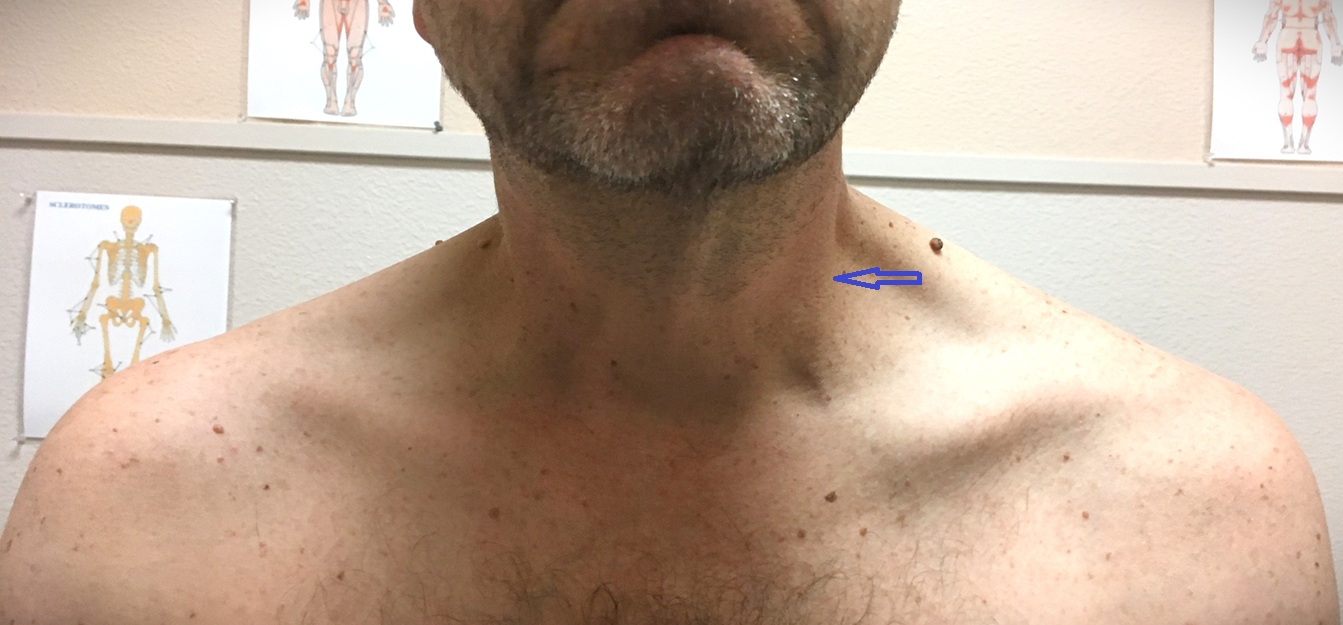
Fig. 1. Anterior neck asymmetry (blue arrow) indicating ASM tension on the left
A close examination of the photograph reveals an apparent asymmetry in anterior neck tension (blue arrow), with the left side visibly more contracted. Because the patient is right-handed, this discrepancy is abnormal. Its location strongly suggests tension in the anterior scalene muscle (ASM).
Palpatory evaluation was performed using Wartenberg’s Test, which confirmed a severe spasm in the ASM. Even minimal pressure applied above the left clavicle triggered acute shooting pain radiating to the thumb and left scapula.
Since the ASM governs the brachial plexus, its irritation fully explains the radiating pain to the thumb. However, the trapezius muscle does not receive motor innervation from the brachial plexus. Instead, it is innervated by the accessory nerve (cranial nerve XI). So, can tension in the ASM provoke acute trapezius spasm despite their different sources of innervation?
Yes. After exiting the skull, the accessory nerve crosses the posterior cervical triangle before entering the trapezius. The anterior and middle scalene muscles form the medial wall of this triangle. A spastic ASM can compress the accessory nerve within this area, producing a reflexive trapezius spasm.
Figure 2 illustrates the anatomy of the posterior cervical triangle and the pathway of the accessory nerve (by TeachMeAnatomy).
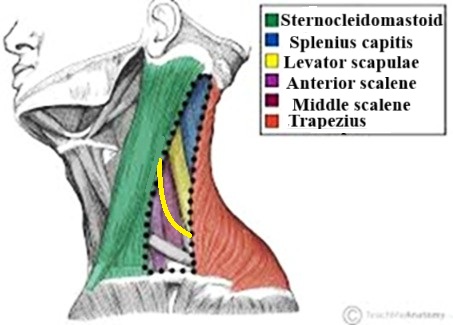
Fig. 2. Anatomy of the posterior cervical triangle and the pathway of the accessory nerve
(bright yellow line)
A DC, a PT, an acupuncturist, and a massage therapist had previously treated our patient. All treatments provided only temporary relief because each practitioner focused primarily on the trapezius and other posterior cervical muscles. This error in the evaluation led health practitioners to treat secondary, compensatory reactions (trapezius spasm) rather than the initial trigger (ASM tension).
Visual observation is only the first step in clinical evaluation. However, in many cases, such as this one, it provides invaluable data. Further examination allowed for the full restoration of the chain of clinical events:
- During the clinical interview (send step in clinical evaluation), the patient recalled a severe episode of influenza accompanied by persistent, forceful coughing.
- As a result, he developed significant tension in the anterior scalene muscle (ASM), which was visible on visual inspection. It compromised the brachial plexus in the anterior cervical region and caused irritation of the radial nerve, producing symptoms in the left upper extremity.
- Because the ASM is part of the posterior cervical triangle, the increased pressure in this region resulted in significant entrapment of the accessory nerve, triggering a severe spasm of the left trapezius muscle.
- The spastic trapezius muscle subsequently increased pressure within the suboccipital space, entrapping the greater occipital nerve and provoking headache symptoms.
Thus, in response to the chronically present initial trigger (ASM spasm), the patient’s brain formed a multilayered chain of compensatory reactions. They obscure the initial trigger, and they dominate the clinical picture. This is why previous treatment attempts failed.
Five sessions of the ASM Medical Massage protocol combined with decompression of the accessory nerve in the posterior cervical triangle fully resolved the patient’s symptoms and restored normal cervical and left upper-extremity function.
CONCLUSION
During SOMI training, we consistently remind therapists that chronic somatic disorders ALWAYS develop according to the “domino principle,” where the actual trigger hides beneath layers of reflex and compensatory reactions developed by the patient’s brain. This case is an excellent demonstration of that concept.
Therapists must learn to read the patient’s body like an open book, identify the initial trigger, and avoid being misled by secondary but sometimes dominant symptoms that mask the real source of dysfunction. This is precisely why SOMI’s instruction in soft-tissue evaluation is a critical foundation for achieving stable, clinical outcomes.
SOMI is seeking clinically oriented therapists who are willing to enter the professionally exciting field of MM to study its theory, soft-tissue evaluation, and the clinical application of MM protocols. Join SOMI for Live Webinar and Hands-on Seminars as a part of the Medical Massage Certification Program and inject clinical science into your practice!
Here is SOMI’s 2026 schedule with 10% off for early registration for each Webinar and Seminar before February 1st: Medical Massage Courses & Certification | Science of Massage Institute » Medical Massage Continuing Education
A great first step is to take a Live Webinar on Medical Massage Theory and Soft Tissue Evaluation on January 17-18. Medical Massage Courses & Certification | Science of Massage Institute » SOMI’s MM Theory Webinar January 17-18, 2026
ABOUT THE AUTHOR

Here is a link to the author’s Bio: Medical Massage Courses & Certification | Science of Massage Institute » Editorial Board
Category: Blog
