
We continue to review how massage therapy heals the human body through various mechanisms, summarized in Diagram 1. We started this discussion in the Jan/Feb (Part I) and Mar/Apr (Part II) 2010 issues of JMS, and we covered cellular stimulation, the phenomenon of piezoelectricity, and streaming potentials.
This and previous articles on the theoretical explanation of mechanisms responsible for the therapeutic power of massage therapy contained a lot of medical terminology and concepts. We recognize that readers may have difficulty reading these articles and effectively using the information they contain.
In JMS, we try to present information in the most useful form, and we strongly believe in the great professional and intellectual potential of our readers. This is why we would like to equip you with as much scientifically updated information as possible. Also, we are sure that it is time for scientific data to replace personal opinions and anecdotal experience, which we frequently see in many massage publications. To enhance the article’s practical value, we included Practical Tips, which we hope will link theoretical information to its clinical application. Also, use data from tour publications to build productive professional relationships with the local medical community. Thus, be sure to pay attention to these parts of the article.
Previously, in issue #3 of JMS, we began discussing scientific data that explains how massage therapy triggers local and general vasodilation. We reviewed how massage therapy affects vasodilation through its mechanical actions, and the effect of ischemic compression on local circulation in the trigger-point area.
In Diagram 1, we summarized the clinical effects of therapeutic massage. We based this schematic on publications that scientifically examined the therapeutic mechanisms of massage therapy. As mentioned above, we have already discussed the impact of therapeutic massage on cellular function and the electrical environment (see the January/February and March/April 2010 issues of JMS). To replay the diagram, please click on the ‘play’ button at the beginning of the sliding bar (blue line) located just below the diagram.
Diagram 1. Local healing mechanisms of massage therapy
In this article, which concludes Part III, we will focus on the reflex mechanisms massage therapy uses to enhance local and general vasodilation. The concept of a reflex mechanism means that the practitioner who uses scientifically based massage techniques can actively involve the client’s nervous system to stimulate local and general circulation. Two major reflex mechanisms that massage therapy uses to stimulate vasodilation are the Axon Reflex and the Central Mechanism of Vasodilation.
AXON REFLEX
Axon reflex is a lesser-known factor responsible for reflex vasodilation. This important information is largely absent from massage publications, yet it has great practical value. We will examine the axon reflex using Diagram 2 below.
The main job of peripheral receptors (touch, pressure, vibration, temperature, pain, muscle spindle receptors, and Golgi tendon organ receptors) in the soft tissue is to report to the CNS any fluctuations in the outside environment or any changes in the local function. If the stimulation of peripheral receptors in the layers of the soft tissue (‘A, B, C, D’ in Diag. 2) is strong enough to reach their threshold, the peripheral receptors form sensory input to the CNS ( ‘F’ in Diag. 2) which is then sent to the posterior horn of the spinal cord (‘G’ in Diag. 2). These parts of the spinal cord work as a sensory computer, and are responsible for the initial processing of arrived data from periperal receptors to determine its nature and level of threat. After initial processing of arrived information, the posterior horns of the spinal cord send information to other parts oof CNS for future evaluation, e.g., to the upper motor center in the brain and to the anterior horns of the spinal cord (‘H’ in Diag. 2) where lower motor centers are located. In both scenarios, the CNS will form so – called motor response (‘I’ in Diag. 2) back to the tissue where peripheral receptors were initially stimulated.
Motor responses result from the upper (cerebral) or lower (spinal) motor centers, which are quite different. In the first case (upper motor centers), a decrease in outside temperature forces one to wear additional clothing, but a person may take some time to decide which exact sweater or jacket to choose before finally putting on additional clothes. In the second case (lower motor centers), cutting the finger elicits immediate motor responses, such as a quick hand withdrawal, to minimize further damage. The obvious difference between the two responses depends on the level of potential damage.
The motor responses also control local and general vasoconstriction/vasodilation. In the first discussed example, response to the lower temperature will trigger chill and ‘goose bumps’ which will be accompanied by local, and eventually general, vasoconstriction. The same reflex vasoconstriction happened after cutting the finger, and its goal is to minimize blood loss and stop bleeding.
When the practitioner places their hands on the client’s body, the initial body response is local reflex vasoconstriction. This is the normal protective reaction of the CNS. If the practitioner continues to apply massage strokes to the affected area and uses the correct massage protocol, the spinal cord will recognize that the activation of sensory receptors in the affected area is harmless, and it will greatly diminish the motor response responsible for the initial vasoconstriction, with the following local vasodilation in the massaged area.
To reinforce vasodilation in the massaged area, the body also employs the Axon Reflex (AR), an important mechanism that the practitioner should use to increase and maintain local vasodilation. Dr. LeRoy (1941) was the first scientist to point to the possible involvement of the AR in local and general vasodilation triggered by massage therapy. Peripheral vasodilation triggered by AR can result from inflammation within the nerve (as a pathological condition) or from repetitive, intense mechanical stimulation of the soft tissues, e.g., massage strokes (Jacobs, 1954). Besides peripheral vasodilation, the AR is responsible for the increase of sweat production as a result of sweat gland stimulation (Schmidt et al, 2011).
Let’s review the AR mechanism using the interactive Diagram 2 below. To start the interactive diagram, please click the ‘play’ button below. To replay the diagram, please click on the ‘play’ button at the beginning of the sliding bar just below the diagram.
Diagram 2. Axon Reflex
First, we will indicate the major anatomical components presented on the diagram. The solid arrow indicates massage strokes.
A – Indicates the skin with peripheral receptors.
B – Indicates subcutaneous tissue with peripheral receptors.
C – Indicates the superficial fascia with peripheral receptors.
D – Indicates the superficial skeletal muscles with peripheral receptors.
E – Indicates the loop of the axon reflex.
F – Indicates the ascending sensory fibers from the peripheral receptors to the spinal cord.
G – Indicates the posterior horn of the spinal cord, which processes sensory information arriving from the peripheral receptors.
H – Indicates the anterior horn of the spinal cord, which controls the motor response to the tissues and organs.
I – Indicates the descending motor fibers from the spinal cord to the soft tissue.
Blue dot – Indicates sensory stimuli that travel from peripheral receptors to the spinal cord.
White dot – Indicates the nerve impulses that travel inside the spinal cord between the sensory center in the posterior horn and the motor center in the anterior horn.
Red dot – Indicates vasodilatory response from the spinal cord to the soft tissue where the peripheral receptors are stimulated.
Green dot – Indicates the pathway of the vasodilatory impulses that travel to the soft tissue using the loop of the axon reflex.
Now, let us put the chain of events into motion (turn on the interactive diagram). When the sensory receptors in the soft tissues are activated by massage strokes, they send signals to the CNS (moving blue dot) using the ascending (i.e., to the spinal cord) sensory fibers of the peripheral nerve (letter ‘F’ on the diagram). After the initial reflex vasoconstriction, the spinal cord begins to recognize massage strokes as harmless and decreases vasoconstriction, triggering vasodilation. This is when the AR kicks in, enforcing vasodilation.
Here is how AR works. Despite the spinal cord ceasing to respond to peripheral receptor input during massage strokes, the peripheral receptors in the massaged areas continue to fire information to the spinal cord. As you can see in the Diagram, small parts of fibers that form the peripheral nerve split from the nerve trunk and form the so-called axon reflex arc (letter ‘E’ on the diagram). These short collaterals connect back to the arterioles and capillaries in the tissue where the peripheral receptors were activated by massaged strokes.
Thus, peripheral receptors continue to send signals to the spinal cord, and some of these signals return to the capillaries and arterioles in the massaged area (a moving green dot), further reinforcing peripheral vasodilation. This vasodilation is more likely triggered by a histamine-released pathway from the neighboring mast cells (Solcanyi, 1996). This additional vasodilation is triggered BEFORE vasodilatory stimuli from the anterior horns of the spinal cord (moving red dot) can reach the arterioles in the massaged soft tissue. In this case, the reflex vasodilation is a result of the combined impact of motor response from the lower motor centers in the spinal cord and the axon reflex.
As several studies have shown, the practitioner may expect vasodilation only if using intense massage techniques. The effleurage alone won’t trigger the AR (Severini and Veranado, 1967). As Hansen and Christiansen (1973) found in a very elaborate study examining vasodilation using 133Xe radioisotope clearance from the skin, subcutaneous, and muscle tissue, effleurage triggers vasodilation only while it is applied. Vasodilation stops in 2 minutes after cessation of effleurage strokes. Vasodilation was observed for a much longer period after the application of percussion and kneading techniques, which are more effective because they also engage the AR.
Carlsson et al. (2006) considered the axon reflex one of the most important vasodilatory mechanisms underlying the clinical outcomes of acupuncture treatment.
Practical Tip 1
Beyond its theoretical importance, the information about AR has great clinical value. To activate AR, the practitioner should use repetitive application of intense stimulating techniques (e.g., friction) to activate peripheral receptors as much as possible and, at the same time, increase histamine levels, which the AR uses as a mediator to trigger peripheral vasodilation.
There is an important issue to keep in mind. Always start working in the new part of the body with effleurage to drain tissues, gradually increasing speed, intensity, and application to more intense affective techniques.
As we discussed above, the body’s initial response to massage strokes in a new area is vasoconstriction. Thus, if the therapist starts with intense techniques, it will prolong the vasoconstriction period and, as a result, the practitioner will lose impact. The initial effleurage helps relieve initial vasoconstriction and prepares the tissue for techniques that will trigger the AR.
CENTRAL MECHANISM OF VASODILATION (CMV)
CMV means that the central nervous system is directly responsible or partly involved in local or general vasodilation. There are three major mechanisms by which massage therapy stimulates vasodilation locally and generally. They are:
- Central inhibition of vasoconstriction
- Vaso-motor reflex
- Viscero-somatic reflex.
Let’s review them separately
Central Inhibition of Vasococontriction (CIV)
Central inhibition of vasoconstriction indirectly supports local and general vasodilation by reducing sympathetic nervous system activity, which predominantly controls the body during daytime hours and under any type of emotional or physical stress. Thus, vasodilation as a result of CIV is a product of decreased vasoconstriction. CIV is one of the keystones of the stress-reduction massage. Medical Massage therapy also relies on this mechanism. For example, the Inhibitory Regime of massage therapy, the initial component of Trigger Point Therapy, uses CIV to optimize treatment effectiveness.
The concept of CIV as a primary component of stress reduction and muscle relaxation was initially formulated in 1939-1940 by Dr. E. Jacobson, based on almost 15 years of experimental and clinical observations. Later, Jacobs (1960) and Valentine (1984) also concluded that massage inhibits the vasomotor center in the brain, decreasing the activity of the sympathetic (stress) division of the autonomic nervous system, which, in turn, plays an important role in vasodilation and the overall decrease in stress levels.
The excellent book on the subject (Korthuis, 2011) summarizes scientific data on blood circulation in the skeletal muscles and also addresses this issue. It is worthwhile to cite.
“The skeletal muscle vasculature is richly innervated by the sympathetic nervous system and exhibits high sympathetic tone in resting conditions. This relatively high level of basal activity, coupled with myogenic tone, maintains the arteries and arterioles supplying skeletal muscle in a partially constricted state. Thus, centrally directed withdrawal of sympathetic tone (bold by JMS) to the skeletal muscle…results in vasodilation.”
Vasomotor Reflexes (VR)
VRs are under the control of the vasomotor center, which is in charge of the peripheral vasoconstriction and vasodilation in arterioles. Thus, these reflexes are directly responsible for blood flow through tissues and inner organs. The vasomotor center is located in the medulla oblongata of the brain (see Diagram 3) and also controls cardiac function, as well as coughing, sneezing, vomiting, and swallowing.
Diagram 3. Medulla oblongata
As we have discussed, VRs are mostly controlled by the sympathetic division of the autonomic nervous (stress) system, and, normally, the arterioles throughout the body are less than 50% of maximal constriction (Bullock et al. 1984). Thus, when we discuss vasodilation, we should primarily refer to the level of vasoconstriction or vasomotor tone (Davis, Hill, 1999; Korthuis, 2011). In such cases, peripheral vasodilation is a direct consequence of reduced normal vasoconstriction or of decreased sympathetic (stress) nervous system activity. In simpler terms, this means massage – inhibition of the vasomotor center – stronger, longer-lasting vasodilation.
The existence of VRs triggered by massage therapy was first demonstrated by Prof. Zabludovsky (1913), who used a plethysmograph to record increased blood flow in the forearm opposite the massaged area and in both calves of the same subject. VRs and their correlation with massage therapy were extensively studied by Ebeland and Wisham (1956). Using various tests, including the rate of radiosodium clearance from the massaged and non-massaged tissues, the authors concluded that massage therapy triggers local and general vasodilation via VRs.
Chernigovsky (1980) conducted extensive research on the function of peripheral receptors, especially baroreceptors, which regulate the degree of constriction/dilation of blood vessels and, consequently, blood flow. At first, the author used massage as one of the tools to study peripheral receptor activity. However, initial data led the author to dig deeper and examine massage therapy as a tool to elucidate its impact on local and general vasodilation.
Based on the experimental data, Dr. Chernigovsky developed a very interesting theory to explain the profound impact of massage strokes on both general and local vasodilation. According to this theory, the body’s capillary network serves as a reflex zone of the entire cardiovascular system. Thus, the upper vasomotor centers, the heart, and all vascular structures, down to the arterioles, adjust their functions in response even to local changes in the capillary network. Dr. Chernigovsky’s work explains the effectiveness of Medical Massage Therapy in the early stages after a heart attack. Here is a logical chain of events:
correctly applied massage strokes – local vasodilation – the entire capillary network responds with reflex vasodilation – decrease peripheral vascular resistance – unload the heart and decrease cardiac work.
Severini and Venerado (1967) showed that applying massage techniques to one leg triggers vasodilation in the opposite leg. The same data was supported by Prilutsky (2003), who conducted a pilot study for the Beverly Laboratory of Vascular Studies in Los Angeles. The author examined the effect of Swedish Massage, applied using various effleurage and Medical Massage, on arterial blood circulation in the lower extremities of healthy adults. Pulse Volume Recording (PVR), Photoplethysmograph, and Thermography were used to compare arterial blood circulation in both groups. The largest changes were registered in PVR. What is important about this study is that all measurements were conducted in the lower extremity opposite to the massaged one. Let’s review the data from one of the subjects.
The study involved two massage practitioners, one who practices Swedish Massage and one who practices Medical Massage. The original PVR value in the lower right extremity of the subject was 0.81. After a 15-minute Swedish massage of the lower left extremity, the PVR on the right dropped to 0.73, indicating that arterial blood perfusion even slightly decreased on the opposite, non-massaged lower extremity. At that moment, the Medical Massage practitioner began working on the same subject for 15 minutes, and the PVR began to climb almost immediately. At the end of 15 minutes, PVR on the unmassaged lower extremity was 1.22. Thus, arterial blood perfusion was almost twice the 0.73 value when the Medical Massage practitioner took over. After treatment stopped, PVR in the unmassaged extremity continued to rise, and at the end of the second hour it was 1.63.
Castro-Sanchez et al. (2011) examined the impact of Connective Tissue Massage on blood circulation in patients with Type 2 diabetes. Ninety-eight Type 2 diabetes patients with stage I or II peripheral arterial disease were randomly assigned to a clinical and control group. Using various tests and equipment, the authors compared blood circulation in the toes of patients with Type 2 diabetes.
Interestingly, the authors tested the effectiveness of Connective Tissue Massage (clinical group) against magnetotherapy (control group) while patients in both groups continued to receive standard medical care for type 2 diabetes. The statistical evaluation of the obtained data allowed the authors to conclude that:
“Connective tissue improves blood circulation in the lower limbs of type 2 diabetic patients at stage 1 or 11-a (P<.05) and may be used to slow the progression of peripheral arterial disease.”
Practical Tip 2
If the practitioner would like to trigger long-lasting vasodilation as a result of therapeutic or stress reduction sessions, he or she should use various kneading and light percussion techniques. The kneading techniques should be applied separately on the level of skin and the level of superficial and deep skeletal muscles.
The effleurage techniques many practitioners rely on in their massage routine are incapable of producing effective and, what is more important, long-lasting vasodilation. Effleurage techniques must be used to drain the tissue, but the practitioner should limit their application. Otherwise, treatment efforts are wasted.
Practical Tip 3
If the practitioner deals with patients who have impaired circulation (e.g., as a result of Diabetes, Thrombosis Obliterans, etc.), he or she should use more sophisticated and effective massage methods to improve blood circulation (e.g., Connective Tissue Massage, Segment-Reflex Massage, Neuromuscular Therapy). In such cases, the practitioner uses Medical massage therapy, specifically designed to address these conditions. In these cases, the practitioner combines local vasodilation with reflexive vasodilation to restore or improve blood supply to the affected areas.
Practical Tip 4
Glezer/Dalicho zones for patients with circulatory abnormalities (discussed below in the Viscero-Somatic Reflexes section) are a great guide for designing an effective massage protocol.
Practical Tip 5
To enhance the vasodilatory effect of medical massage, the practitioner should always start treatment on the opposite, unaffected part of the body, which matches the exact location of the affected area. In such cases, the practitioner first uses reflex vasodilation to prepare for work in the affected area and improve local circulation.
Viscero-Somatic Reflexes (VSR)
Another way massage therapy enhances vasodilation is via VSRs. These reflexes are the foundation for the application of Medical Massage in cases of chronic inner organ disorders. These reflexes link soft tissues (skin, fascia, skeletal muscle, and periosteum) with the affected inner organ. VSRs are possible because the soft tissue structure and inner organs share innervation provided by the same segment of the spinal cord.
For example, the same segments of the spinal cord are responsible for the innervation of the lungs, skin, and fascia in the posterior neck and middle back, trapezius muscle, and periosteum of the scapula. Thus, health practitioners may expect that patients with chronic pulmonary abnormalities (e.g., emphysema) will exhibit pathological changes, such as reflex zones, in these areas of the body. The presence of reflex zones in soft tissue is one of the driving forces behind the progression of pulmonary abnormalities.
English physician Dr. H. Head formulated the concept of VSRs and, in 1893, published maps of possible skin abnormalities associated with various visceral disorders. These maps, known as Head’s zones, are classic examples of VSRs. Other maps were later published (e.g., Dicke’s maps), but the most comprehensive work was done by two German physicians, Dr. O. Glezer and Dr. V.A. Dalicho, who, in 1953, published what they called Glezer/Dalicho’s zones.
Diagram 4 presented below shows Glazer/Dalicho zones in cases of chronic pulmonary disorders. It indicates the most common locations of pathological abnormalities, in the form of reflex zones, in the soft tissues of patients with chronic pulmonary disorders. Dr. Glezer and Dalicho published diagrams for every system of the human body, as well as the most common location of somatic abnormalities.
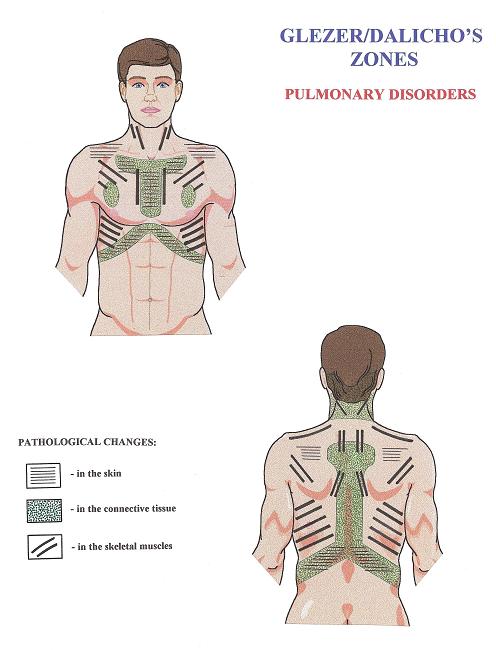
Each set of diagrams shows the location of reflex zones in the skin (parallel thin lines), connective tissue (dotted areas), and skeletal muscles (parallel thick lines). The existence and participation of VSRs in the control of inner organ function as well as VSR’s importance as therapeutic pathways on normalization of the affected inner organs are reported by numerous studies (Korr, 1947; Ebner, 1956; Beal, 1985; Johnston and Golden, 2001; Giamberardino, 2003; Giamberardino et al, 2005; Jarell, 2009; Desmaris et al, 2011).
The practitioner who uses correctly formulated MEDICAL MASSAGE PROTOCOL is able to eliminate pathologically developed reflexes in the soft tissue and, at the same time, normalize the function of the affected inner organ by restoring its normal innervation and triggering long-lasting vasodilation, which helps to mobilize the reparative abilities of the tissue of the affected organ.
Practical Tip 6
If the practitioner would like to optimize therapy and prioritize the client’s interests, the applied massage treatment must be formulated and adjusted individually. It is a professional mistake to apply massage to all clients without making personal modifications based on each client’s health needs. Otherwise, the massage session becomes senseless rubbing.
Let’s say the therapist works at the spa, and a new client is scheduled. Usually, the therapist asks every new client about soft tissue abnormalities and possible chronic visceral disorders. Equipped with such basic data, the practitioner must consider the location of the reflex zones associated with the client’s chronic visceral abnormality according to Glezer/Dalicho zones. In such cases, the practitioner adjusts the therapeutic massage routine based on the location of reflex zones in the soft tissues.
By focusing on reflex zones and emphasizing their importance to the client, the practitioner prevents reflex zone formation or reduces their intensity. Even the simple fact of spending more time in these areas makes a big difference to the patient’s health.
If the therapist practices Medical Massage, the diagnosis of visceral abnormalities allows participation in the treatment of the chronic visceral disorders using specially designed Medical Massage protocols. In these cases, the use of Medical Massage becomes complex due to the highly effective interplay between local and reflexive mechanisms.
Having witnessed the results of medical massage therapy for patients with chronic visceral disorders in our clinic, we believe that clinically effective application of MEDICAL MASSAGE PROTOCOLs in cases of chronic visceral disorders is the highest level of the massage therapist’s expertise. Of course, this is the author’s personal opinion.
If you are on the East Coast, don’t miss SOMI’s first 2026 hands-on training in Soft Tissue Evaluation and three Medical Massage Protocols, in Fayetteville, NC, on March 6-8: Medical Massage Courses & Certification | Science of Massage Institute » Fayetteville, NC March 6-8, 2026
Beal M.C. Viscerosomatic reflexes: a review. JAOA, 85(12):53-58, 1985
Bullock J., Boyle J., Wang, M.B., Ajello, R.R. Physiology. ‘John Wiley Sons’, Pennsylvania, 1984
Carlsson CP, Sundler F, Wallengren J. Cutaneous innervation before and after one treatment period of acupuncture. Br. J. Dermatol, 155: 970-976, 2006
Castro-Sanchez A.M., Moreno-Lorenzo C., Mataran-Penarrocha G.A., Feriche-Fernandez-Castanys B., Granados-Gamez G., Quesada-Rubio J.M.Connective tissue reflex massage for type 2 diabetic patients with peripheral arterial disease: randomized controlled trial. Evid Based Complement Alternat Med., 2011: 804321, 2011
Chervigovsky V.N. Interoreceptors. ‘Medicina’, Moscow, 1980
Davis M.J., Hill M.A. Signaling mechanisms underlying the vascular myogenic response. Physiol Rev., 79: pp. 387-423, 1999
Desmaris A., Descarreaux M., Houle S. Piche M. Tuning the gain of somato-sympathetic reflexes by stimulation of the thoracic spine in humans. Neurosci Lett., Feb 25;490(2):107-11, 2011
Ebel A., Wisham L.H. Effect of massage on muscle temperature and radiosodium clearance. Arch. Phys. Med., July: 339-405, 1952
Ebner M. Peripheral vasculatory disturbances: treatment by massage connective tissue in reflex zones. Br. J. Phys. Med., 19(18):176-180, 1956
Gelzer O. Dalicho V.A. Segmentmassage. Leipzig, 1955
Giamberardino M.A. Referred muscle pain/hyperalgesia and central sensitisation.J Rehab. Med., May;(41 Suppl):85-8, 2003
Giamberardino M.A., Affaitatti G., Lezra R., Lapenna D., Costantini R., Vecchiet, L. Relationship between pain symptoms and referred sensory and trophic changes in patients with gallbladder pathology. Pain, Mar;114(1-2):239-49, 2005
Hansen T.I., Kristiansen J.H. Effect of massage, short wave diathermy and ultrasound upon 133Xe disapperance rate from muscle and subcuteneous tissue in the human calf. Scand J Rehab Med., 5:179-182, 1973
Head H. On disturbances of sensations with special reference to the pain of visceral disease. Brain, 16:1-133, 1893
Jacobs M. Massage for the relief of pain: anatomical and physiological considerations. Phys.Ther. Rev., 40: 93-98, 1960
Jacobson E. Variation of Blood Pressure With Skeletal Muscle Tension and Relaxation. Ann. Interal Med., 12:1194-1212, 1939
Jacobson E. Variation of Blood Pressure With Skeletal Muscle Tension and Relaxation. Ann. Interal Med., 13:16-19-1625, 1940
Jarrell J. Demonstration of cutaneous allodynia in association with chronic pelvic pain. J. Vis. Exp., Jun 23;(28), 2009
Johnston W.L., Golden W.J. Segmental definition–Part IV. Updating the differential for somatic and visceral inputs. JAOA, May;101(5):278-83, 2001
Korr I.M. The neural basis of the osteopathic lesion. JAOA, 47(4): 191-198, 1947
Korthuis RJ. Skeletal Muscle Circulation. San Rafael (CA), Morgan & Claypool Life Sciences, 2011
LeRoy R. Le vie du tissu conjonctif et sa defense par le massage. Rev. de Me. Paris, 58: 212, 1941
Schmidt R., Weidner C., Schmelz M. Time course of acetylcholine-induced activation of sympathetic efferents matches axon reflex sweating in humans. J Peripher Nerv Syst., 16(1): 30-36, 2011
Severini V., Venerando A. The physiological effects of massage on the cardiovascular system. Europe Medicophysica, 3:165-183, 1967
Szolcsanyi J. Neurogenic inflammation: reevaluation of axon reflex theory. In:Neurogenic Inflammation, Edited by Pierangelo Geppetti and Peter Holzer. ‘CRC Press’, 33-43, 1996
Valentine K.E. Masage in psychological medicine – modern use of an ancient art.New Zeland J. Physiotherapy, 12:15-16, 1984
Zabludovsky I.V. Massage Techniques. ‘Medicina’, St. Petersburg, 1913
ABOUT THE AUTHOR

Here is a link to the author’s Bio: Medical Massage Courses & Certification | Science of Massage Institute » Editorial Board
Category: Medical Massage
