
This clinical case was submitted to the Journal of Massage Science by SOMI’s recent graduate of the Medical Massage Certification Program, Troy Flathau, LMT, CMMP.
The uniqueness of this case lies in the complexity and combination of somatic pathologies that developed within the patient’s body, manifesting as both local and reflex abnormalities. A therapist’s primary responsibility is to identify the initial trigger of somatic dysfunctions and not be misled by secondary reflex reactions that frequently mask the true source of the problem.
Please also pay close attention to the remarkably small number of sessions Troy required to completely eliminate chronic somatic abnormalities after multiple traditional therapies had failed to produce lasting clinical results.
Dr. Ross Turchaninov, Editor-in-Chief
SEVENTEEN-LEVEL SPINAL FUSION AND POSTTRAUMATIC ANTERIOR SCALENE SYNDROME VS. MEDICAL MASSAGE
By Troy Flathau, LMT, CMMP
Jeddo, MI
When I first met this patient in May of 2024, I did not yet realize how much this case would reshape my clinical thinking.
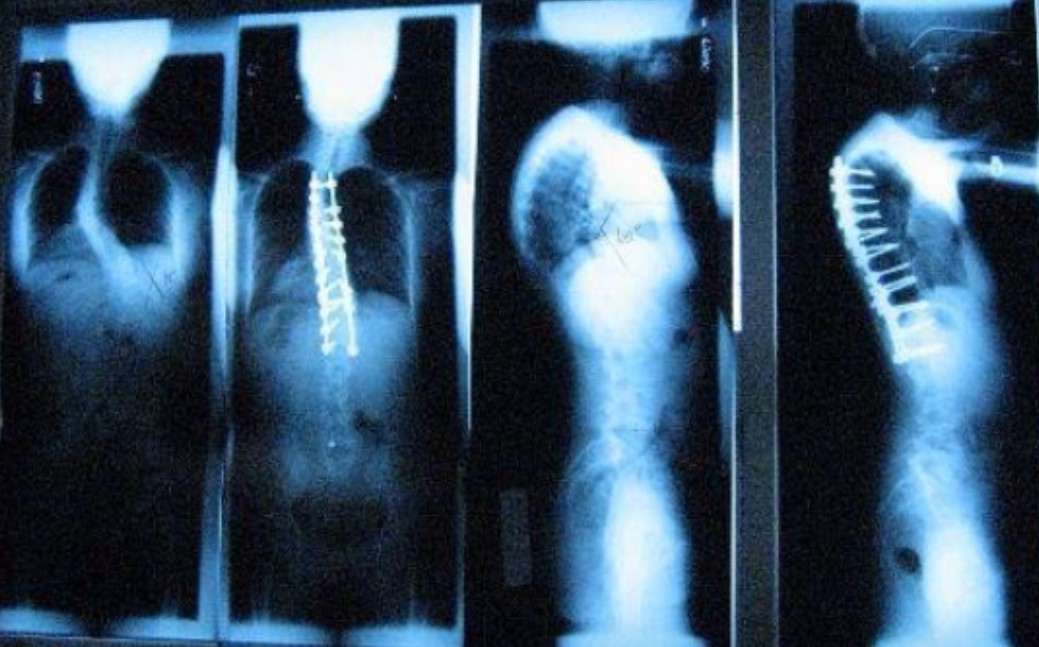
She was a 40-year-old female with a long and complicated medical history. Diagnosed with scoliosis during adolescence, she had undergone two major spinal surgeries that resulted in fusion from C6 to L3—seventeen spinal levels in total. Despite these interventions, she had lived with pain for most of her life. Over time, she had adapted psychologically to her condition to such an extent that her perception of pain no longer followed a normal scale. What most patients would describe as severe pain, she had learned to call “manageable.” For her, a 6 out of 10 was considered a good day.
Figure 1a illustrates the initial severity of her scoliosis and the results of the first spinal surgery to fuse cervical and thoracic vertebrae. Fusion of lumbar vertebrae was performed later during the second spinal surgery.
The patient is left-handed, works in the medical field, and spends long hours at the computer—factors that would later prove to be clinically significant.
At the time of our evaluation session, she presented with two major complaints. The first was an acute, deep, sharp pain in the left posterior shoulder. The pain intensified with arm elevation and was particularly severe at night, often disrupting her sleep. At times, it was so intense it would take her breath away.
The second complaint was chronic left elbow pain, accompanied by significant loss of grip strength. This had been ongoing for almost four years following a motor vehicle accident.
At that stage in my career, my understanding of peripheral nerve involvement and the formation of reflex zones was still limited. I approached her shoulder pain as a local issue. I identified severe superficial and deep fascial restrictions throughout the posterior cervical region and shoulder. Palpation revealed an active trigger point in the left rhomboid minor, which appeared to restrict the function of the trapezius muscle.
Drawing on what I had learned from early exposure to the Science of Massage Institute’s publications, I decided to apply a structured, layer-by-layer approach to soft tissue rehabilitation.
1st session
I started with drainage of the posterior neck and shoulder, followed by work on the superficial fascia using Skin Rolling, Skin Kneading, and Connective Tissue Massage. I then applied the Lateral Shift Technique to decompress the deeper fascial layers between the trapezius and rhomboids. Once tissue mobility improved, I proceeded with Trigger Point Therapy targeting the rhomboid minor. I carefully control the degree of applied pressure without overstepping the patient’s pain threshold.
The patient reported an immediate reduction in pain intensity after the session, and we scheduled a follow-up.
2nd session
The patient informed me that the next day, she experienced a severe flare-up—so intense that she considered going to the hospital. Ultimately, she chose not to, anticipating that she would only be prescribed pain medication. Interestingly, by the following morning, the sharp pain had disappeared. She had mild soreness, but her range of motion had significantly improved.
3rd Session
The patient didn’t have a reaction to the previous Medical Massage therapy session the next morning. No more shoulder pain, and she was starting to get good sleep. Encouraged by this progress, I continued with the same treatment I used during the previous session, but added the Post-isometric Relaxation Technique.
In three sessions of Medical Massage, I was able to completely alleviate her shoulder pain, restore normal ROM, and return her to normal sleep! Three sessions had accomplished what months of discomfort had not.
At that point, I was eager to address her elbow pain, but the patient was hesitant. She feared that any intervention might worsen her condition, as previous treatments had done. Respecting her concerns, I continued to provide supportive care for her shoulder and back.
By May of 2025, her elbow pain had reached a point where she began seriously considering surgery. The patient agreed to let me address it first, and by then, I felt even more confident because I was a third of the way through my Medical Massage Certification with SOMI and had developed much better assessment and treatment skills.
ELBOW AND ARM EVALUATION
Her history revealed a complex progression. Following the car accident in 2021, she initially developed symptoms consistent with Cubital Tunnel Syndrome (irritation of the ulnar nerve in the cubital canal), including numbness in the ring and pinky fingers. She underwent ulnar nerve transposition surgery, which provided significant relief.
However, during the following PT rehabilitation, she developed lateral elbow pain, eventually diagnosed as Lateral Epicondylitis (a.k.a. Tennis Elbow). Despite multiple steroid injections, physical therapy, and various self-care strategies, her condition in the left lateral elbow continued to deteriorate. By the time I re-evaluated her, she had been living with this pain for nearly four years.
This time, my clinical approach was different. Knowing that the radial nerve innervates the lateral elbow, I examined its origin and potential sites of compression. Thus, instead of focusing on the elbow itself, I began tracing the radial nerve pathway as I learned from SOMI.
Cervical Compression Test to examine potential disk problems and the Compression Test of paravertebral muscles were negative. However, when I performed Wartenberg’s Test on the anterior scalene muscle, the patient immediately reported pain radiating down to her elbow. That moment changed everything!
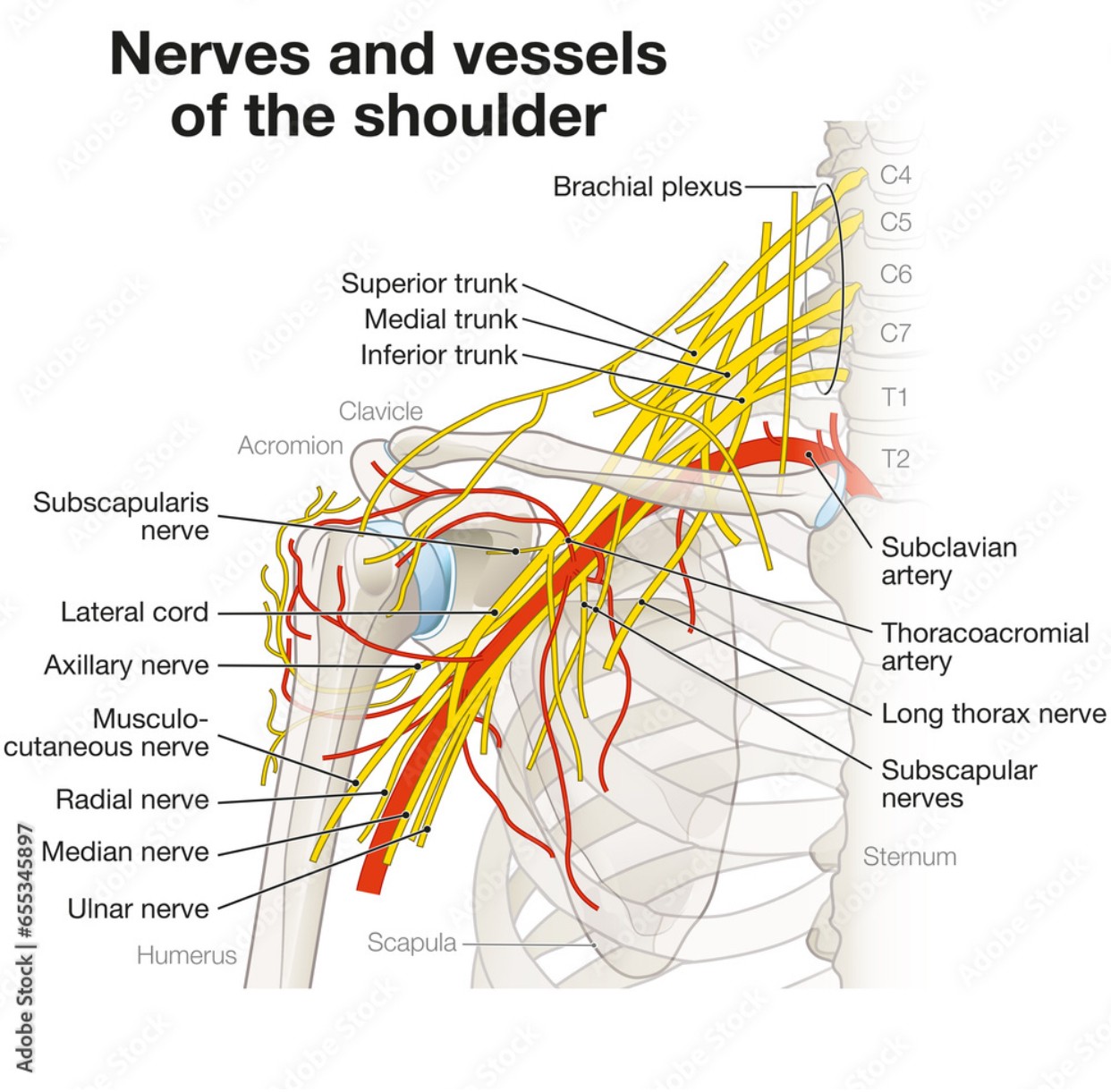
It became clear that the radial nerve was being irritated proximally—at the level of the brachial plexus—due to tension in the anterior scalene muscle. The elbow pain was not the primary problem, but rather the result of a larger pathological chain of reflex reactions. Fig. 2 illustrates the anatomy of the brachial plexus.
Further assessment confirmed fascial restrictions in the forearm and an active trigger point in the supinator muscle. However, I understood that treating these local findings without first addressing the origin of radial nerve irritation would not lead to lasting results.
1st session
I started with brachial plexus decompression using the Anterior Scalene Muscle Medical Massage Protocol. I then addressed the forearm fascia and applied Trigger Point Therapy to the supinator.
At the end of the session, the patient looked at me, formed a tight fist, and said, “Look—I can squeeze without pain.” It was the first time in years she could do that!
2nd session
Two days later, during the second session, Wartenberg’s test was negative. The nerve irritation had subsided. I continued to stabilize the anterior neck and focused the remainder of the session on restoring mobility in the forearm tissues.
3rd session
By that time, the patient was completely pain-free. Grip strength had returned, and normal function was restored. I added gentle radial nerve stretching to support long-term recovery.
Ten months later, she remains pain-free and has full functional use of her arm. Looking back, the mechanism of her abnormality becomes clear to me. The initial trauma from the seatbelt likely caused hypertonicity of the anterior scalene muscle, which, in turn, compressed the brachial plexus. This irritation affected the radial nerve, altering both sensory (to the brain) and motor (from the brain) signaling. The result was a cascade of dysfunction—protective muscle tension, decreased circulation, and ultimately the formation of trigger points in the forearm.
What presented as a local elbow problem was, in reality, a manifestation of a proximally located radial nerve irritation by the anterior scalene muscle. However, the irritation was mild, and the patient did not report any neck symptoms. In such a case, her Tennis Elbow was a pure reflex reaction, which everyone missed, focusing instead on the elbow itself.
LESSONS LEARNED
For me, this case clinically reinforced critically important training in Medical Massage I received from SOMI, and now I fully appreciate it:
- When we understand which nerve(s) control the part of the body experiencing chronic somatic abnormalities, we can clinically trace all possible triggers from the level of the disk where it originates, all the way to the affected area
- We must eliminate peripheral nerve irritation, if present, before treating soft tissue locally, or we will never achieve stable clinical results.
- The patient must be fully willing to cooperate with their recovery process for the best results. Otherwise, the patient’s anxiety state due to the chronic pain will limit the treatment process.
- Previous failed treatment strategies from other healthcare providers don’t mean that we will fail in our treatment. As my clinical experience now shows in these cases, Medical Massage IS the defining treatment strategy for restoring the patient’s health. Even in this clinical case, the only solution my patient was offered was an elbow surgery. However, FOUR YEARS of pain and failed therapies were resolved in THREE SESSIONS of Medical Massage!
- We must stop chasing the pain! We must correctly identify the trigger and eliminate it with the correct Medical Massage protocol. This is why Science of Massage Institute’s training in Medical Massage is such a vital part of our profession!
REFERENCES
- DeStafano, Lisa, Principles of Manual Therapy, 5th Edition
- Turchinanov, Ross, M.D., Medical Massage Volume 1, 2nd Edition
SOMI is seeking clinically oriented therapists who are willing to enter the professionally exciting field of MM to study its theory, soft-tissue evaluation, and the clinical application of MM protocols. Join SOMI for Live Webinars and Hands-on Seminars as part of the Medical Massage Certification Program. We share with you only clinically effective, independently tested methods and modalities, and teach you how to combine them to achieve the ultimate clinical results. As all SOMI’s former students, you will build up a completely new and efficient practice based on clinical science!
Here is SOMI’s 2026 schedule: Medical Massage Courses & Certification | Science of Massage Institute » Medical Massage Continuing Education
Hands-on Training in Medical Massage protocols in Longwood, Florida, on July 11-13. Medical Massage Courses & Certification | Science of Massage Institute » Longwood, FL July 11-13, 2026
Program:
Saturday: Medical Massage Techniques Hands-On Training Course
Sunday: Medical Massage Protocol for Pectoralis Major and Minor Muscles Syndrome
Monday: Medical Massage Protocol for Piriformis Muscle Syndrome/Sciatica
Don’t miss SOMI’s Live Webinar on Medical Massage Theory and Soft Tissue Evaluation on August 1-2: Medical Massage Courses & Certification | Science of Massage Institute » SOMI’s MM Theory Webinar August 1-2, 2026
ABOUT THE AUTHOR

Chronic and complex pain conditions are a frustrating and confusing puzzle. Helping people solve that puzzle is the focus of my work.
I have always been drawn to asking the deeper “why” to any problem. I carry that mindset into my Medical Massage education at the Science of Massage Institute and now into my practice, which integrates my clinical experience since 2016 with strong scientific evidence and the unique individualized approach to treating each patient who comes to my clinic.
If you want more than short-term relief, then O.S. Bodywork in Port Huron, Michigan, is where that process begins:
troyflathaumassage@yahoo.com
615-500-7099
Category: Case Studies
Tags: 2026 Issue #1
